Incidental Durotomy/ Dural Tear ICD-9-CM Coordination and Maintenance
24 Slides7.57 MB
Incidental Durotomy/ Dural Tear ICD-9-CM Coordination and Maintenance Committee March 19-20, 2008 John D. Shaw, President, Next Wave, Albany, NY
Objectives Define ‘dural tear’ (‘incidental durotomy’) Differentiate dural tears from other accidental punctures or lacerations I.D. Risk factors that increase likelihood of dural tears during spine surgery I.D. Reporting Bias (significant underreporting by Hospital and/or MD) Discuss Coding Options and Guidance for classifying incidental dural tears 2
Background Dural tear is often associated with intricate surgical procedures on the spine Given the delicate anatomy of structures operated on, it is often not avoidable despite meticulous technique Pre-existing comorbidities (diabetes, steriod use, smoking, et. al) increase risk Pre-existing deformities (scoliosis/kyphosis, spondylolithesis, stenosis) increase risk 3
Incidental Durotomy/Dural Tear Definition: Consequence of Unrepaired Dural Tear: Small tear in the dura mater Often unavoidable occurrence of spinal surgery Ideally identified and repaired inter-operatively. Further CSF leak Formation of pseudo-meningocele Impact on Post-Operative Care: Patient experiences CSF headache (349.0) Increased Nursing Care (monitoring, strict orders for ‘head on bed’ for 24 hours or longer) 4
Dural Tears: Coding Issues USE of ICD-9-CM: Disproportionate Impact on Common Quality Indicator (AHRQ PSI-15), Note: Spine Surgery Removed (Version 3.2, March 2008) until Two Refinements to Address Bias Completed: 1-Consistent ICD-9-CM Reporting across hospitals 2-Refined Risk Adjustment (AHRQ and MD team) Major Systematic Under-Reporting Bias (Address Today) Large & Predictable Variation in Patient Risk High Variability in Risk between Hospitals General vs. Specific Coding Guidance Differences 5
Systematic Under-Reporting Bias AHRQ is Removing Spine Surgery Cases from PSI-15 until coding bias is addressed (V.3.2) 46% of 2,446 Hospitals Performing Spine Surgery Report NO Dural Tears at all (MEDPAR) Surgeons in Some of These Hospitals Have Journal Articles Reporting Dural Tear Rates Close to 10% Many Hospitals Report Repair of the Dural Tear, but NOT the Dural Tear Itself 57% of Hospitals Performing Spine Surgery Significantly Under-Report 6
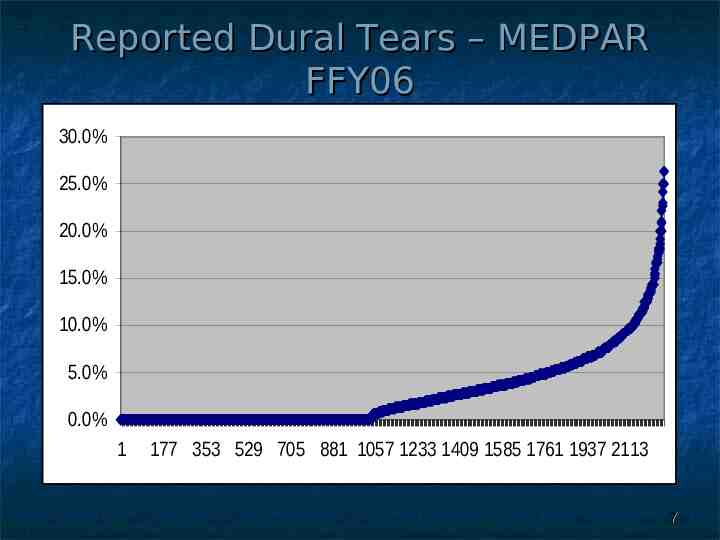
Reported Dural Tears – MEDPAR FFY06 30.0% 25.0% 20.0% 15.0% 10.0% 5.0% 0.0% 1 177 353 529 705 881 1057 1233 1409 1585 1761 1937 2113 7
Disproportionate Impact on Common Quality Indicator (AHRQ PSI-15) 13% of 998.2 – Accidental puncture or laceration during a procedure, but 40% of Variation Between Hospitals 34% of Hospitals do not do Spine Surgery 25% of Spine Surgery Concentrated in 5% Huge Impact on Current Quality Rankings Future Concerns – Pay for Performance 8
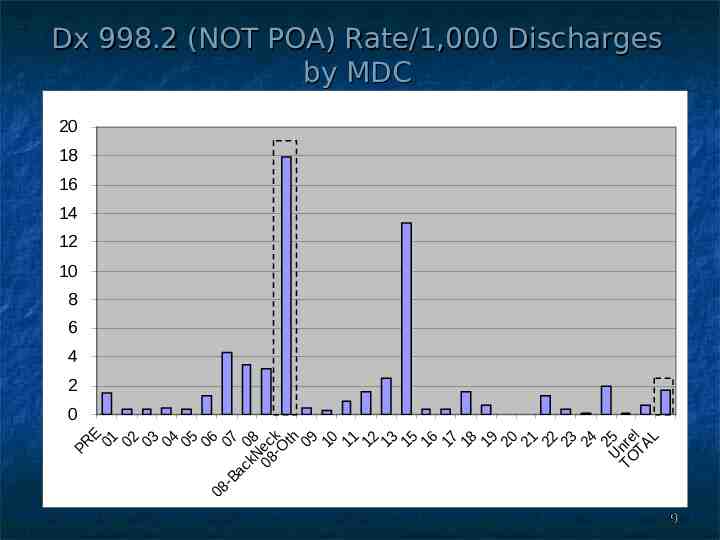
Dx 998.2 (NOT POA) Rate/1,000 Discharges by MDC 20 18 16 14 12 10 8 6 4 2 0 E 1 2 3 4 5 6 7 8 ck th 9 0 1 2 3 5 6 7 8 9 0 1 2 3 4 5 rel L R P 0 0 0 0 0 0 0 0 Ne -O 0 1 1 1 1 1 1 1 1 1 2 2 2 2 2 2 Un TA O k 08 T c Ba 08 9
Dural Tear Risk Factors Diagnosis – Type and Location of Spine Condition Patient Anatomy – Mechanics Type of Surgery – Fusion, Laminectomy, Disk Removal Comorbidities – Prior Surgery, Predictors of Thinning Dura, etc. 10
Data on Dural Tear Administrative Data reports less than half of rates reported in clinical literature Wide Reporting Variation Across Hospitals Results of Recent Multi-Facility Trial: SPORT Spondylolysthesis (NEJM 5/07) Lumbar Stenosis (NEJM 2/08) Random Cohort: 11% Observational Cohort: 9% Random Cohort: 8% Observational Cohort: 10% Disk Herniation (JAMA 11/06) Random Cohort: 4% Observational Cohort: 2% 11
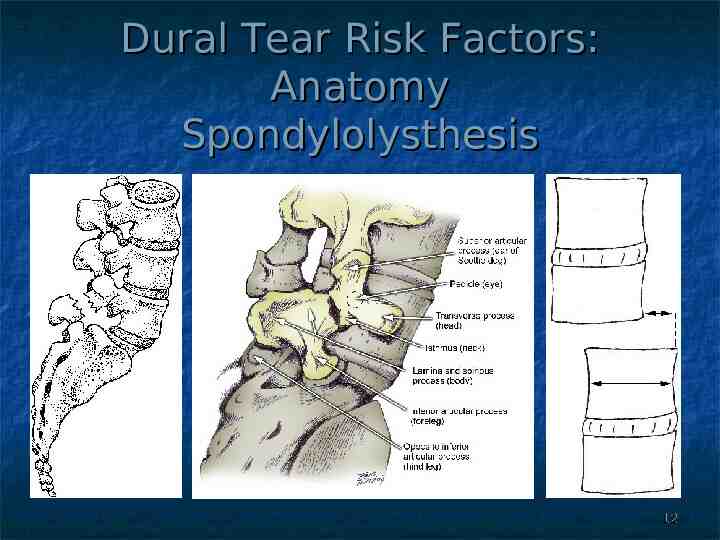
Dural Tear Risk Factors: Anatomy Spondylolysthesis 12
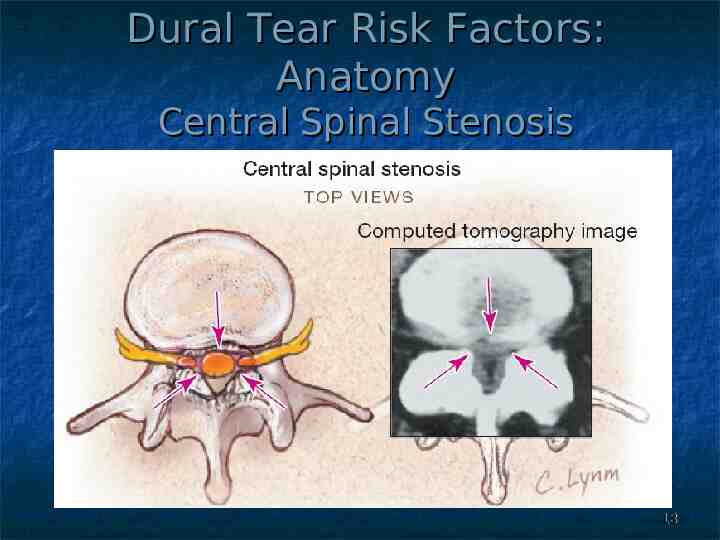
Dural Tear Risk Factors: Anatomy Central Spinal Stenosis 13
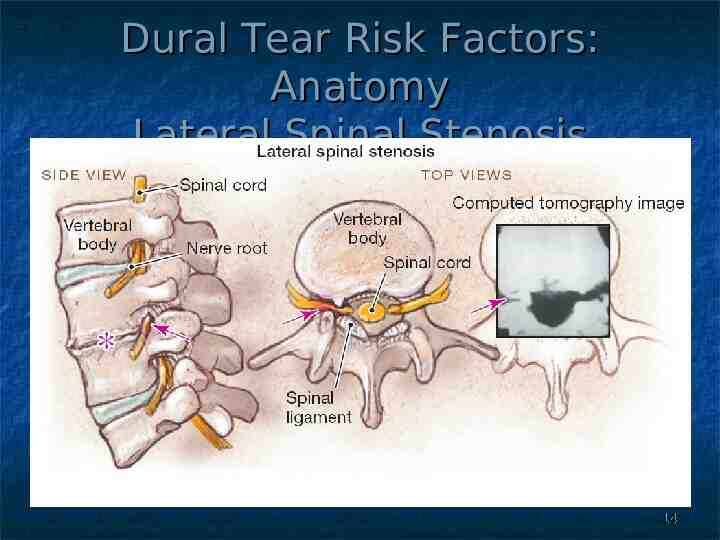
Dural Tear Risk Factors: Anatomy Lateral Spinal Stenosis 14
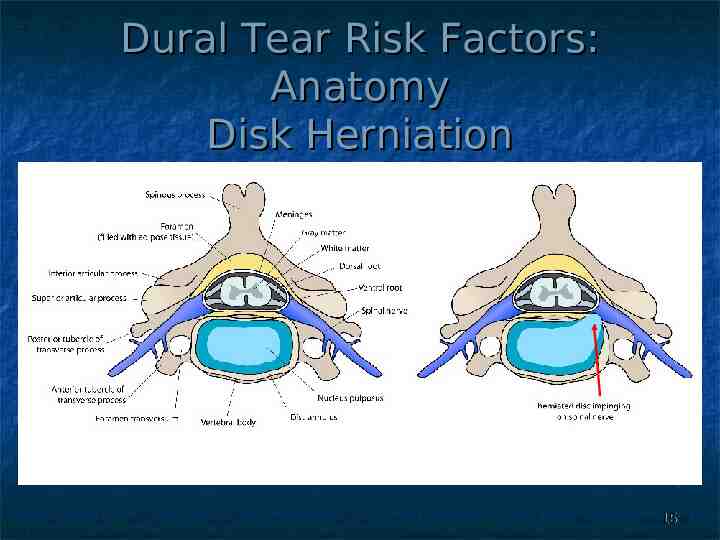
Dural Tear Risk Factors: Anatomy Disk Herniation 15
Expected Dural Tear Frequencies: by Type of Surgery Revision Spine Surgery: 15 – 33% Multi-Level (3 ) Spine Surgery: 13 – 15% “Other” Spine Surgery: 7 – 10% Single Level Fusion: 7 – 8% Two Level Decompression: 4 – 5% One Level Open Diskectomy: 2 – 4% Single Level Decompression: 0 – 1% 16
Dural Tear Risk Factors: Other Comorbidities Meningeal Adhesions (349.2) Exostosis (Osteophytes) (721.8) Diabetes (250.00 – 250.93) Obesity (278.00-278.01, V85.30-V85.4) Chronic Steroid Use (V58.65) Smoking (305.1, V15.82) Kyphosis or Scoliosis (737.10-737.9) 17
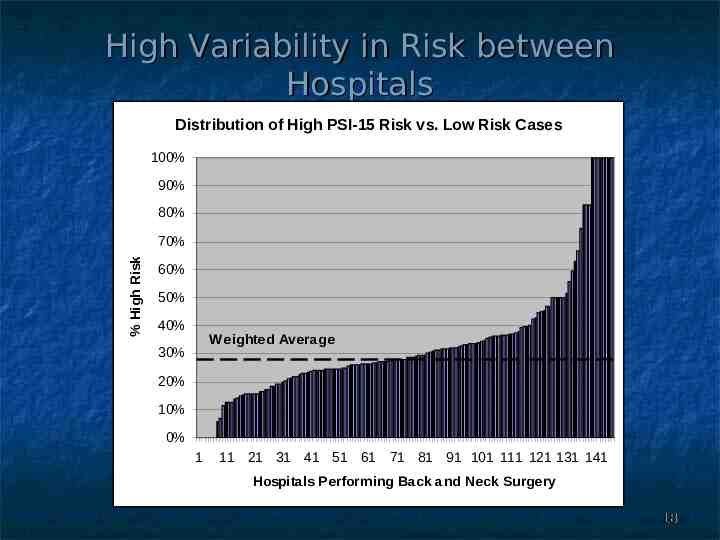
High Variability in Risk between Hospitals Distribution of High PSI-15 Risk vs. Low Risk Cases 100% 90% 80% % High Risk 70% 60% 50% 40% Weighted Average 30% 20% 10% 0% 1 11 21 31 41 51 61 71 81 91 101 111 121 131 141 Hospitals Performing Back and Neck Surgery 18
Coding Incidental Dural Tears SHOULD be Coded as Additional Diagnosis Repair, Increased Monitoring, Extended Stay SHOULD be Differentiated from Punctures or Lacerations that Don’t Affect Stay WHERE to Code is A Major Issue Complications of Multiple Body Sites 996-999 Currently Indexed to 998.2 Conflict: MD Must Document as “More Than Routinely Expected Complication”, but Considers Dural Tear to be Common/Incidental/Unavoidable Specific Body Site ICD-9-CM Default 19
AHA (Faye Brown) ICD-9-CM Coding Handbook - Chapter 29 (Emphasis added) “Categories 996 through 999 are provided in ICD-9-CM for complications of medical and surgical care that are not classified elsewhere. Note that all conditions that occur following surgery or other patient care are not classified as complications. First, there must be a more than routinely expected condition or occurrence. . the fact that the problem is a complication due to a procedure must be documented by the physician; the coder cannot make this determination. . . Complications of surgical and medical care are classified in ICD-9-CM as follows: Complications that occur only in other specified body sites are classified in that chapter of ICD-9-CM Complications that affect multiple sites or body systems are generally classified in category 996-999 20
Coding Clinic and Index Coding Clinic First Quarter 2006 Page15: Question: What is the appropriate code for a dural tear that occurs during surgery? Answer: Assign code 998.2, Accidental puncture or laceration during a procedure, for a dural tear that occurs during surgery. Dural tears are usually inadvertent, but fairly common in re-do spinal surgery where the dura has thinned out. (Emphasis added) October, 2007 ICD-9-CM Code Book tear, dural is now officially indexed to code 998.2 21
Coding Options Option 1 – New 5th Digit in 998.2 998.20 Accidental puncture or laceration during a procedure, unspecified site 998.21 Accidental puncture or laceration of dura during a procedure 998.29 Accidental puncture or laceration during a procedure, other specified site Option 2 – Code to Body System (preferred) 349.3 Dural Tear (incidental) (spinal) (vertebral) (cerebral) (thoracic) (lumbar) 22
Code Also (Both Option 1 or 2) Code Also Associated Conditions Adhesions, meningeal (349.2) Diabetes (250.00-250.93) Exostosis (Osteophytes) (721.8) Obesity (278.00-278.01) (V85.30-V85.4) Intervertebral Disc Disorders (722.0-722.9) Kyphosis or Scoliosis (737.10-737.9) Post Laminectomy Syndrome (722.83) Spinal Stenosis (724.00-724.09) (723.0) Spondylosis (721.0-721.91) Spondylolithesis (756.10-756.19) Steroids (V58.65) Tobacco Use Disorder (305.1), (V15.82) 23
Precedents for Option 2 AHA/Faye Brown’s ICD-9-CM Coding Handbook (Chapter 29) – added between 1999 and 2003 “Complications that occur only in other specified body sites are classified in that chapter of ICD-9-CM” Specific Precedents Back to 1995 Iatrogenic hypotension moved from 997.91 to 458.2 Iatrogenic pulmonary embolism code moved from 997.3 to a new 5th digit 415.11 (Iatrogenic PE) 24