Diagnosis and Management of Psoriasis and Psoriatic Arthritis SIGN







30 Slides610.00 KB
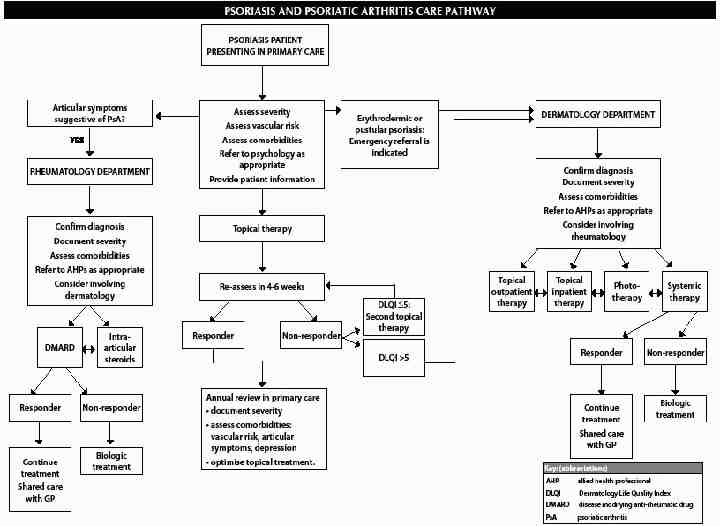
Diagnosis and Management of Psoriasis and Psoriatic Arthritis SIGN November 2010
Objectives According to this new guideline: Be able to diagnose psoriasis Know the recommended treatment in primary care Have an understanding of psoriasis management in secondary care.
What are the characteristics of psoriasis?
What risks are associated with psoriasis or psoriatic arthritis?
Co Morbidities associated with psoriasis Diabetes Hypertension Hyperlipidaemia Metabolic syndrome Obesity MI – young pt with severe disease. Low mood
Treatment - Topical Short term potent steriod or potent steriod plus calcipotriol gain improvement in plaque psoriasis. Long term treatment is a Vit D Analogue. If unsuccessful then consider dithranol, coal tar solution or tazaotene gel.
Vitamin D analogues Calcipotriol and talcalcitol. Dovonex, silkis, curatoderm. Dovobet (with betamethasone) Analogues of vit D and affect cell division and differentiation Do not smell or stain
Coal Tar Anti-inflammatory properties and antiscaling properties. Crude coal tar most effective, but not tolerated due to smell and mess. Contact allergy or folliculits may occur. Polytar, alphosyl HC, Cocois
Tazarotene For plaque psoriasis. A retinoid. Less effective and more irritation than calcipotriol. Use sparingly on plaques only. Clean and odourless.
Dithranol Effective treatment for plaque psoriasis. Irritation and staining of the skin. Only on plaques. Not in flexures or on the face. Wear gloves to apply and wash afterwards. Best used by specialist nursing staff.
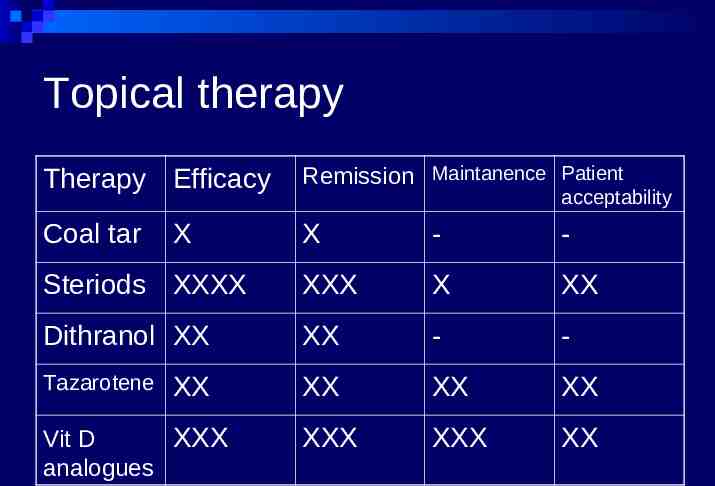
Topical therapy Therapy Efficacy Remission Maintanence Patient Coal tar X - - Steriods XXXX XXX X XX Dithranol XX XX - - Tazarotene XX XX XX XXX XXX XX X XX Vit D XXX analogues acceptability
Special Sites Scalp – scalp preparations – salicylic acid / tar preparations. Vit D analogues and steriods Face and Flexures – more easily irritated. Moderate steriods short term Vit D Analogues or tacrolimus ointment.
Assessing Psoriasis PASI - calculated based on severity, intensity, and surface area Requires experience at calculating the score. DLQI Simple 10 questions, assess effect on life.
Dermatology Life Quality Index 0-1 no effect at all on patient's life 2-5 small effect on patient's life 6-10 moderate effect on patient's life 11-20 very large effect on patient's life 21-30 extremely large effect on patient's life
Referral to dermatology Diagnostic problem Extensive disease Occupational disability / time lost Difficult places Failure of topical therapy Adverse reaction to topical DLQI above 6
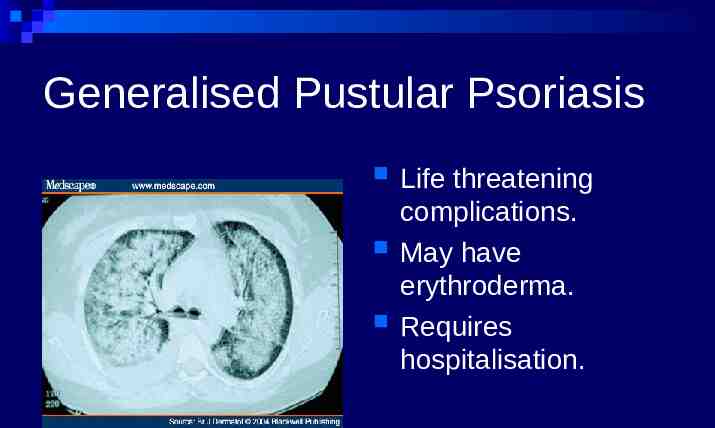
Generalised Pustular Psoriasis Life threatening complications. May have erythroderma. Requires hospitalisation.
Secondary Care Erythroderma or generalised pustular psoriasis need emergency referral to dermatology. These patients should have inpatient care.
Secondary Care - Phototherapy Narrow band UVB phototherapy should be offered if failure to topical therapy. Three times weekly where practical
Systemic In general poor studies to go on and of short duration. However, Severe or refractory psoriasis pt should be offered tx with ciclosporin, methrotrexate, acitretin. If respond – shared care with primary care.
Biological Strong evidence base for infliximab (NNT 2) adalimumab, and etanercept (NNT 4). Should be offered to pt who do not respond to systemic therapies.