Adverse Childhood Experiences (ACE’s) Trauma informed care and




24 Slides915.32 KB
Adverse Childhood Experiences (ACE’s) Trauma informed care and what this means for me Bite sized session for any practitioner who wants to know more Cheryl Beirne, Angela Ladocha and Louise Seddon 12.11.2020
WARNING This video may well relate to you on a personal level. If you feel that you need support to deal with any issues that this video highlights for you, Locala wants to help. Locala provides Restorative supervision Clinical supervision Coaching Employee Assistance Programme
What do you already know about ACE’s Work in pairs and discuss what you already know about ACE’s Come back and share with the group one thing you know already and one thing you hope to find out
Learning outcomes from this session We hope you will have a deeper understanding about ACE’s and the impact they have on individuals health and well being To have a clear understanding of how the ACE’s study impacts on our work and what this means for everyone who works in a caring / supportive role
What is an ACE . - Physical/Verbal/Sexual Abuse. Emotional/Physical Neglect. - D.V/Parental Separation/Mental illness/Incarceration/ Alcohol/Drug abuse/Incarceration. - 4 ACE’s - Associated with HHB and poor mental health. (Bellis et al, 2015).
The IMPACT .A PUBLIC HEALTH DISASTER - Poor life-course health and social outcomes. - Employ health harming behaviours. - Anger leading to violence. - Poor educational attainment/outcomes/employment. - Risk of early pregnancy, 18 years. - Incarceration. - Lowered mental well-being and life satisfaction. - Inter-generational transmission of ACE’s.
VIDEO CLIP OVERVIEW of ACE’s Wider determinants of Health and further research called “ Adverse Childhood Experiences Study” (ACES) https://www.bing.com/videos/search? q ACEs&&view detail&mid 8520C7767C9C09B370198520C7767C9C09B3701 9&rvsmid 42E524C0E4C6C8457B2842E524C0E4C6C8457B28&FORM VDQVAP
Group work, 4 groups to explore the impact of ACE’s Social impact of ACE’s Physical impact of ACE’s Economic impact of ACE’s Psychological impact of ACE’s Feedback your group findings
LOCKED IN . - Prolonged exposure to stress in childhood can result in children being locked into a high state of alert. - Permanently prepared to respond to further trauma. - Constant state of alert. - Increased tissue inflammation. - Body unable to repair itself. - Poor emotional regulation. - Difficulty controlling impulses. - Poor social interaction. - Employ unhelpful coping mechanisms – Drinking/smoking/drug misuse.(Harris, 2015).
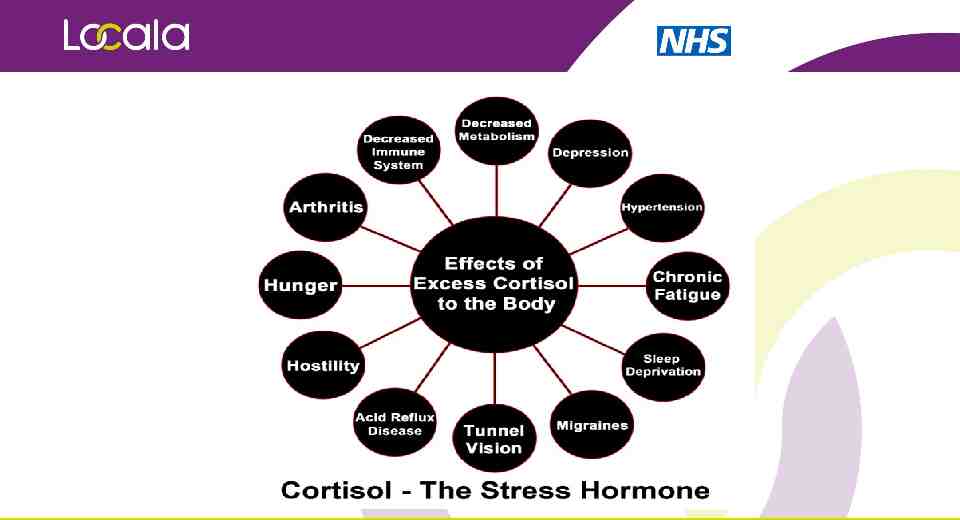
Science and the impact on behaviours HYPOTHALAMUS/PITUITARY AND ADRENAL GLANDS accessed repeatedly to produce fight or flight. ADRENALINE & CORTISOL production and the impact of this on the body (see next slide) NUCLEAS ACCUMBENS – Pleasure/reward centre which is implicated in substance misuse. PRE-FRONTAL CORTEX – Impulse control and learning. AMYGDALA – Mediates fear response.
We need to consider: This study was actually not searching for ACE’s, and the findings were a bi-product of a study that set out to identify root causes of obesity. It became very apparent, very quickly that very ordinary people had suffered a number of ACE’s The study did not look at socio-economic factors, child upon child abuse (bullying), female to male abuse, prescription drug use The authors of the study asked for this study to not be used as a scoring tool for assessment Rather, ACEs to be used as an explanatory factor for a population approach, was never meant for use with individualised care.
Trauma informed services A trauma informed approach for all means Cultural shift not a treatment model – we consider that everyone has suffered some trauma Core principle of DO NO HARM TRAUMA AWARENESS EMPHASIS ON SAFETY REBUILDING CONTROL STRENGTHS BASED ‘Trauma informed care is a strengths-based framework that is grounded in an understanding of and responsiveness to the impact of trauma, that emphasises physical, psychological, and emotional safety for both providers and survivors, and that creates opportunities for survivors to rebuild a sense of control and empowerment’. (Hopper et al (2010) Shelter from the storm, p.82)
Universal Pre-cautions to be applied Group work Discuss in your group how you might apply a universal approach to take into account that everyone you may come across has ACE’s
Client centred care 1.The client is the expert on their own life. 2.Focus on strengths. 3.Follow the client’s heart’s desire. 4.Clients identify solutions that work for them. 5.Only a small change is necessary.
Build on strengths Recognising strengths builds confidence. The recognition, affirmation and celebration of the achievement of planned small steps is empowering and builds self-efficacy. Describe and believe in their own strengths, potential and successes Acknowledge the impact of their own positive efforts Identify their strengths and successes and talk positively with them about their potential.
I can understand that Trauma is an illness of not being able to be fully engaged with the present’ It is a CAN’T not a WON’T. The behaviours that are problematic for us, are solutions to them (such as smoking, alcohol/drug use, over eating, under eating, self neglect, hoarding etc) We, no matter how lovely we are, present a threat. Once anxiety is triggered then a range of defensive weapons are activated – aggression, avoidance, splitting. Seeing past these behaviours is key to building engagement.
Looking beyond a smoking gun Big traumas can be distracting. Sometimes trauma is not the presence of a negative, but the absence of a positive. Poses a problem for insight as many will say they had a ‘happy childhood’ and feel they are just weak/inadequate. Experience of trauma is moderated by access to secure attachments, attuned responses, social supports. It’s really important not to make assumptions about which aspect of a person’s experience has been traumatic.
What to do with a “disclosure” of a trauma? We need to be aware of our emotional reactions to disclosures. People are much more vigilant of our reactions than we think. We can be healing with the small things we do and we can be wounding. When recounting a traumatic event people often focus on the reactions of others, moments of kindness, understanding and moments of callousness. Remembering, asking, listening, soothing, holding in mind. These are things we can all offer. Self-reflection activity, consider a time when you have observed or dealt with a disclosure, how did this go, how did you re-act, what went well, could you have done any thing differently?
Re-cap Affirm that it was a good thing to tell Do not try to gather all the details Ask if the person has told anyone before – and how did that go Offer support (make sure you know what is available) Ask whether the client relates the abuse to their current difficulties Check current safety – from ongoing abuse Check emotional state at end of session Offer follow-up/‘check-in’ Consider reporting
Help individuals understand that the experiences they had may have had an impact on their well We often talk to people about their health conditions, explaining their asthma or being diabetes, but we do not necessarily do the same for mental health and trauma. Individuals are often left wondering what is wrong with them. Just being more informed and aware of why their emotions go up and down, whey they get suddenly scared and angry is the first step to recovery. Doing this without eliciting blame is important, it’s about understanding how my experiences have affected me, not blaming my mother/father for all my problems.
Reference page 1. Felitti http://bigthink.com/videos/vincent-felitti-on-childhood-trauma 2. Unhappy child unhappy adult: http://www.bbc.co.uk/programmes/b070dksr 3. TedMed; How childhood trauma affects health across a lifetime Nadine Burke Harris: https://www.youtube.com/watch?v 95ovIJ3dsNk 4. Centers for Disease Control and Prevention: https://www.cdc.gov/violenceprevention/acestudy/index.html 5. Downloadable PDF versions of most of the ACE Study papers: http://www.theannainstitute.org/ACE%20STUDY%20FINDINGS.html 6. Hillis S D, Anda R F, Dube S R, Felitti V J, Marchbanks P A & Marks J S. The Association Between Adverse Childhood Experiences and Adolescent Pregnancy, Long-Term Psychosocial Consequences, and Fetal Death. Pediatrics 2004;113;320-327