WALKING THE WALK Promoting and Applying Person-Centered Recovery











46 Slides7.45 MB
WALKING THE WALK Promoting and Applying Person-Centered Recovery Concepts Kris Wright, MS, LCPC, RYT
LEARNING OBJECTIVES How Peers can work with consumers, families, natural supports and clinical supports to identify and facilitate progress on personcentered goals and objectives. Promoting exploration and discovery as critical components of holistic, person-centered plans and services. Influencing interdisciplinary teams’ meaningful use of recovery oriented language and their application of recovery concepts to team members’ treatment plans and interventions. Using key concepts in using Person-Centered Care Planning (PCCP) to foster work on recovery goals consistent with consumers’ hopes and dreams and to collaborate with natural and clinical supports. Questions? Don’t hesitate to
TAKE A MOMENT TO REFLECT In your roles, when is easy to advocate for people’s wants, needs, and preferences? When is it harder? And for your own?
PCCP OVERVIEW WARM UP 4 Write 3 goals/areas of meaning you have for yourself on a piece of paper. Hand that paper to the person sitting next to you
RECOVERY A FUZZY CONCEPT Or Should We Say Discovery Everyone recognizes overall meaning different connotation for different people Core elements of concept are clear but unclear on the periphery Can be difficult to operationalize in measurable elements
RECOVERY VS. DISCOVERY
WHAT IS RECOVERY? Patricia Deegan’s definition of recovery: “ The need is to reestablish a new and valued sense of integrity and purpose within and beyond the limits of the disability; the inspiration is to live, work and love in a community in which one makes a significant contribution.” Deegan, P. (1988) Recovery: The lived experience of rehabilitation. Psychosocial Rehabilitation Journal. XI (4) 11-19
RECOVERY is possible for people with mental illness and/or substance use. is different for each person. means that they have a successful, high quality of life even though they have a mental illness. means that they could maintain a job, have friends, go to school, or have a home. may mean that they experience symptoms everyday, but can manage them and still do the things they want to do. Recovery does not mean that they are cured!
THE ULTIMATE GOAL OF RECOVERY-ORIENTED TRANSFORMATION A healthcare system that promotes whole health Consumer and family driven — each adult and child will have access to a full spectrum of integrated services needed to support their wellness/recovery vision Focuses on wellness/recovery — a strengths-based approach to help each person experience health, independence, self-esteem, and a meaningful life in the community Builds resilience — the ability to face life’s challenges and maintain health
THE RECOVERY PLAN AS A ROAD MAP Provides hope by breaking a seemingly overwhelming journey into manageable steps for both the provider and the person served B C D A “life is a journey not a destination” E 10
KEY PRACTICES: THE PROCESS OF PLAN DEVELOPMENT Person is a partner in all planning activities/meetings Provide advance notice Agree upon location Person has reasonable control over logistics Time, invitees, etc. Person offered a written copy Education/preparation regarding the process and what to expect Encourage participation by person’s support network/family Language as a key practice
Consider Structure & Roles in Planning Meetings Treatment Team members arrive on time; introductions The person is given the team’s full attention, e.g., cell phones are turned off; there are no side-bar conversations The person is not “talked about” during the meeting. All comments and questions are directed first to the individual and are a collaborative exchange between the person and his/her Treatment Team. Eliciting the person’s goal (vision/hopes) for their life via a strengths based inquiry “What comes next” is explained to the person, including an opportunity for them to review the plan; provide input
BUILDING A PLAN Outcomes Interventions/Action Steps Short term Goals/Objectives Strengths/Barriers Desired Results/Goals Prioritization Understanding Assessment Request for services 13
A PLAN IS ONLY AS GOOD AS THE ASSESSMENT
WHEN ASSESSMENTS DIFFER . team members disagree about what may be behind what is going on or there are differences in team members’ assessments of how individuals are doing in different parts of their lives odds are they are operating from different information! What can you do?
www.alipar.org Observations: Poor eye contact, unresponsive to social cues, preoccupation with parts of things. Rule Out: ASD Plan: Encourage client to explore part-time employment opportunities such as lawnmower repair or 16
Observations: Recurrent depressed mood leading to breakdowns, social relationships strained by control issues Rule Out: MD w/PF Plan: Encourage to practice social skills building with family connections, consider part-time employment opportunities in seasonal
My battles with addiction definitely shaped how I am now. They really made me deeply appreciate human contact. And the value of friends and family, how precious that is.
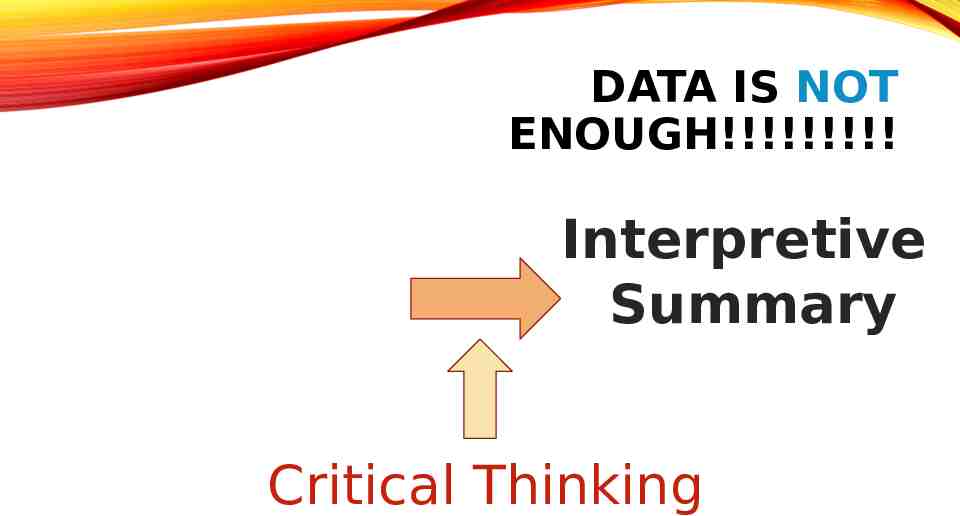
DATA IS NOT ENOUGH!!!!!!!!! Assessment Intake Data Interpretive Summary Critical Thinking
THE IMPORTANCE OF UNDERSTANDING Data collected in assessment is by itself not sufficient for service planning
Assessment Critical Thinking Plan
HYPOTHESES 22 Critical Thinking sometimes generate questions more than answers Helps prioritize and sequence services to fit the individual’s unique needs Best guess about what’s going on Identifies important information that is not known Important for dual diagnosis or when multiple factors are present Example: “It’s not clear whether irritability and aggression are caused by substance use, manic symptoms or a combination of both.”
UNDERSTANDING BARRIERS What is getting in the way of the person achieving their goal(s)? Why can’t they do it tomorrow Why can’t they do it themselves Our focus is removing/reducing/resolving barriers that are a result of the mental illness: symptoms and functional impairments Describe the impact the barriers has on client’s recovery. WHY does the client need support? Describe the challenges that are reaching the client from reaching their goals. What gets in the way? Specify where the client’s behavioral health symptoms and
EXPLORING BARRIERS If there are both mental health symptoms and substance use, discuss the interaction What symptoms constitute warning signs for relapse – when a client is doing well, or does not acknowledge current symptoms, what was going on when things were at their worst? Specify how the barrier or need impacts the client’s life, not just that it exists and IS impacting them. What interventions and activities help? Now? In the past? What are expectations from treatment and what does the client believe his/her responsibilities are?
“NOT EVERYTHING THAT IS FACED CAN BE CHANGED, BUT NOTHING CAN BE CHANGED UNTIL IT IS FACED” JAMES BALDWIN, THE CROSS OF REDEMPTION: UNCOLLECTED WRITINGS
STRENGTHS If we allow despair to take over, we have no strength left in order to do anything at all. Thich Nhat Hanh
The plan: A RECOVERY PLAN SHOULD BE STRENGTH BASED explicitly asks for strengths and interests focuses on the positive, supports the ability to have dreams revolves around achieving goals rather than addressing deficits Strengths are identified by the person, the provider, and also natural supporters/collaterals where appropriate and may include: environmental factors that will increase the likelihood of success identifying the person’s best qualities/motivation strategies already utilized to help competencies/accomplishments interests and activities, i.e. sports, art
SETTING PRIORITIES AND CRAFTING GOALS A NEGOTIATION
NEGOTIATIO N “YOU KEEP USING THAT WORD. I DO NOT THINK IT MEANS WHAT YOU THINK IT MEANS”
GOALS ON PLANS Reflect the client’s needs and hopes (not yours) Short, pithy, to the point, memorable statements of WHAT the client wants to achieve. Worded in positive terms Long term, global, broadly stated with a target date at least a year, perhaps more, in the future. Provides a life change as a result of treatment Based upon their strengths, needs, or preferences Appropriate to stage of change Linked to discharge/transition plans Culturally Sensitive
RESPECTING CULTURAL VARIABLES IN GOAL SETTING The context of an individual’s worldview will impact the desired results process Providers must always remain curious and open to investigate the cultural aspects of developing desired results
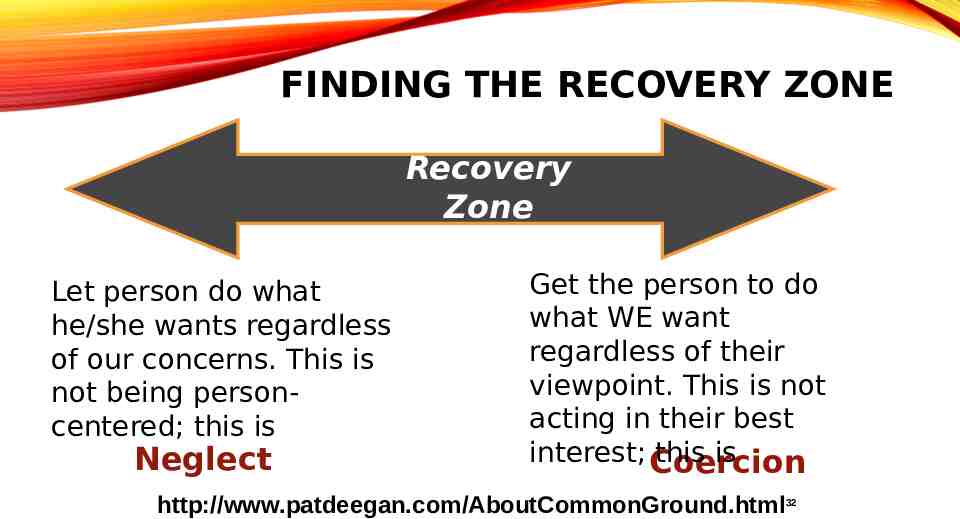
FINDING THE RECOVERY ZONE Recovery Zone Let person do what he/she wants regardless of our concerns. This is not being personcentered; this is Neglect Get the person to do what WE want regardless of their viewpoint. This is not acting in their best interest; Coercion this is http://www.patdeegan.com/AboutCommonGround.html32
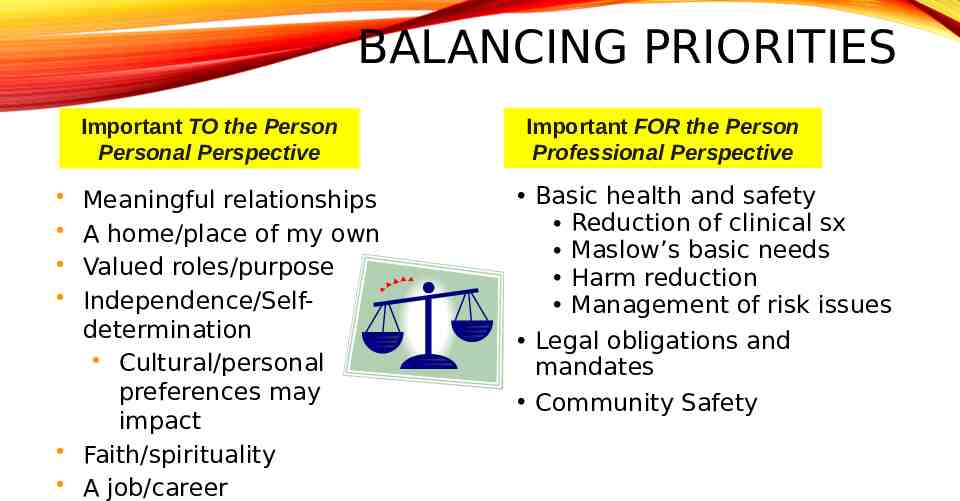
BALANCING PRIORITIES Important TO the Person Personal Perspective Meaningful relationships A home/place of my own Valued roles/purpose Independence/Selfdetermination Cultural/personal preferences may impact Faith/spirituality A job/career Important FOR the Person Professional Perspective Basic health and safety Reduction of clinical sx Maslow’s basic needs Harm reduction Management of risk issues Legal obligations and mandates Community Safety
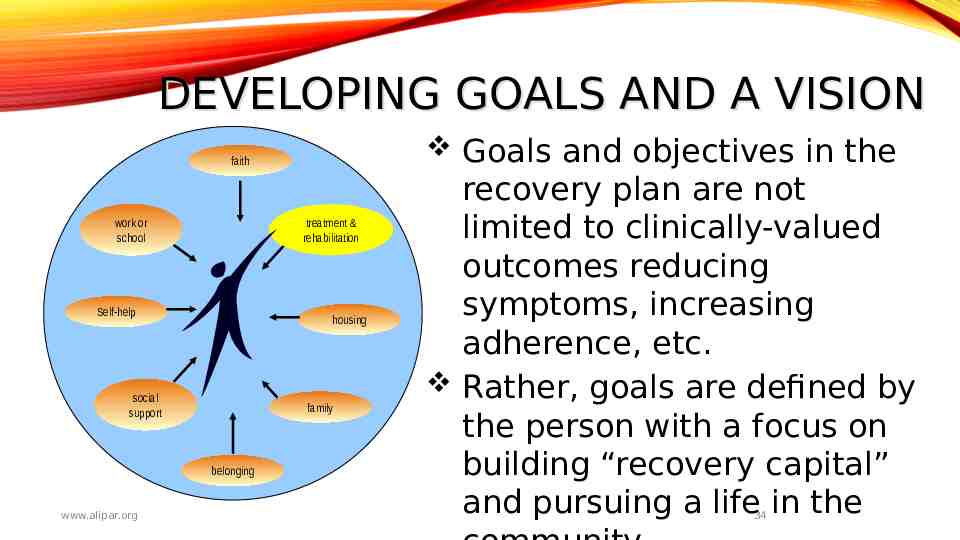
DEVELOPING GOALS AND A VISION Goals and objectives in the faith treatment & rehabilitation work or school Self-help housing social support family belonging www.alipar.org recovery plan are not limited to clinically-valued outcomes reducing symptoms, increasing adherence, etc. Rather, goals are defined by the person with a focus on building “recovery capital” and pursuing a life in the 34
“IT IS A STRANGELY IRRATIONAL NOTION THAT THERE IS SOMETHING IN THE VERY FLOW OF TIME THAT WILL INEVITABLY CURE ALL ILLS. WE MUST COME TO SEE THAT HUMAN PROGRESS NEVER ROLLS IN ON WHEELS OF INEVITABILITY. IT COMES THROUGH THE TIRELESS EFFORTS AND PERSISTENT WORK OF MEN ” DR. MARTIN LUTHER KING JR. LETTER FROM THE BIRMINGHAM JAIL
TEACHING METHODS THAT WORK:
BIG STEPS LITTLE STEPS Objectives: address barriers to the goal by breaking larger goals into expected near-term changes describe changes in behavior, function, or status relate back to functional impairments are understandable for the person served and the team identify key changes that the consumer wishes to accomplish, such as skill building/coping mechanisms address medical necessity Reflect the person’s age, culture, developmental stage Services are not an objective!! 38
What Needs to Be ccomplished to Achieve the Goa
Use your resources! Ideas may include: Skills Building Psychoeducation Accessing Resources Practicing Coping Skills Applying Skills in New Settings Networking Exploration
OBJECTIVES These are the smaller, incremental steps needed to reach the long term goal There should be enough objectives to the duration of the plan, but target dates should make sense Objectives should be clear and measurable so that its obvious to all when the objective has been achieved
SERVICES & ACTION STEPS Services & action steps include those “interventions” provided by professionals which respect individual choice and preference are tailored to the stage of change/recovery describe medical necessity by clearly describing how services are intended to overcome that individual’s barriers are specific to an objective But they also incorporate actions by natural supporters and the person him/herself. 42
ACTION STEPS BY THE PERSON IN RECOVERY & NATURAL SUPPORTERS Traditional plans include only those interventions performed by staff. The recovery model, however, emphasizes the responsibility of a person to participate actively in his or her own care as well as the benefits of seeking contributions of “natural supports” (e.g., family, friends, advocates, & community supporters) For each objective, consider specifying: “Personal Actions” (this promotes a sense of self-agency and helps to activate people in their recovery) and “Natural Support Action” (to help the person build/expand their natural recovery network as a supplement to professional services)
HOW ARE WE FEELING? What seems easy? What seems challenging?
THANK YOU!!!! For more information or with questions visit: The Maryland Behavioral Health website, sign-up and look for “Being Person-Centered” by Diane Grieder (Module 18). CEUs offered. https://mdbehavioralhealth.com/