Supporting the student on clinical placement – academic





61 Slides2.84 MB
Supporting the student on clinical placement – academic and professional practice CLINICAL SUPERVISOR, CLINICAL ASSESSOR, PRACTICE ASSESSOR, PRACTICE SUPERVISOR BSC (HONS) DIAGNOSTIC RADIOGRAPHY CHRIS M ALVEY PROGRAMME LEADER JANUARY 2019
Welcome CPD based refresher and update event Outline of sessions Learning outcomes Course materials Any questions?
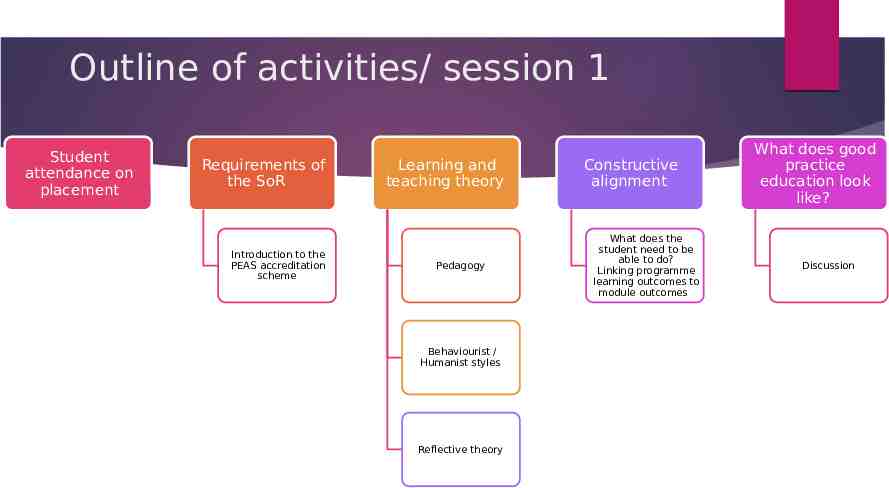
Outline of activities/ session 1 Student attendance on placement Requirements of the SoR Introduction to the PEAS accreditation scheme Learning and teaching theory Pedagogy Behaviourist / Humanist styles Reflective theory Constructive alignment What does the student need to be able to do? Linking programme learning outcomes to module outcomes What does good practice education look like? Discussion
Learning Outcomes 1 By the end of these sessions 2 You will be comfortable with the educational terminology used 3 4 Have a deeper understanding of your role and responsibilities with regards to student placement experiences Know when, to whom, and how to escalate concerns
Student attendance on placement Over the course of the programme, students will spend approximately 40% of the time on placement This will closely follow the existing arrangements with the other education provider, so shouldn’t be too disruptive to existing staff expectations. Precise arrangements for the supervision of students whilst on placement will be the responsibilty ultimately of the placement educator (site) / or education lead for the Trust. They will also be responsible for construction of the weekly placement roster (in cooperation with the University Placement Lead for the programme). The education lead (or equivalent) will be responsible for the day to day maintenance of the roster and will be able to authorise site to site transfers and day swaps / personal leave without recourse to the University Placement Lead for the programme. The University Placement Lead for the programme, will be available for guidance as required to support clinical staff. Clinical assessment is different to what you may be expecting, students are expected to achieve competence in 5 examinations in year 1, these are outlined in the placement documentation. Students should be encouraged to expand the skill set beyond these 5 examinations though
Student assessment - logistics Only staff whom have attended the CPD sessions (this one) will be able to sign off students as competent. We anticipate that this will be restricted to registered practitioners who have been qualified for 18 months or longer. Where, due to operational restrictions, this is not possible, then any band 5 radiographer can sign off any competency, however, this will need to be countersigned by a named clinical assessor or placement / education lead. If students are not able to achieve the required competency, then, it will be acceptable to use practice simulation and a thorough discussion will suffice, this should be indicated within the paperwork In terms of day to day supervision, then any registered member of staff may act as a supervisor (this will satisfy the requirements of IR(ME)R 2018. There is a flowchart in the attached documentation which outlines the process for clinical assessment.
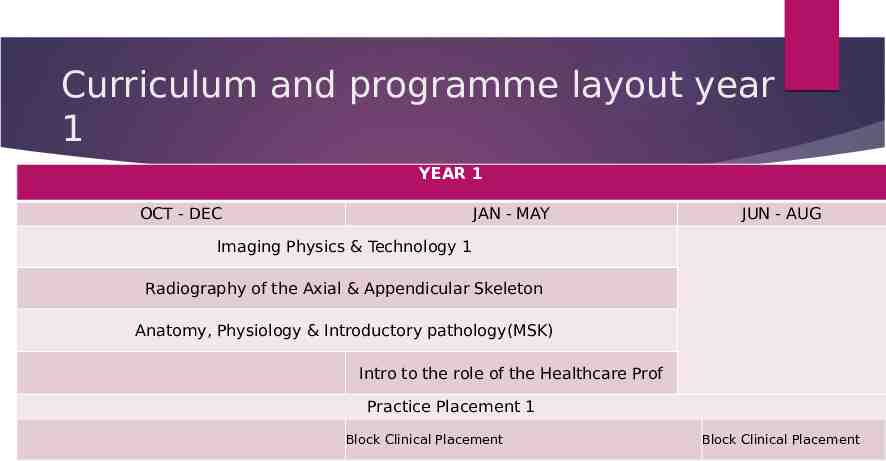
Curriculum and programme layout year 1 YEAR 1 OCT - DEC JAN - MAY JUN - AUG Imaging Physics & Technology 1 Radiography of the Axial & Appendicular Skeleton Anatomy, Physiology & Introductory pathology(MSK) Intro to the role of the Healthcare Prof Practice Placement 1 Block Clinical Placement Block Clinical Placement
Overview of year 1 Week 1 to 9 (September 30th to 25th November) - Academic Week 10 to 19 (2nd December to 3rd Feb) - Clinical placement Week 20 to 37 (10th Feb to 8th June) - Academic (includes 2 weeks holiday and 1week exam/ assessment) Week 38 to 45 (15th June to 3rd August) - Clinical placement Week 46 to 50 (10th Aug to 7th Sep) - Exam / Holiday / recovery of missed placement or reassessment of failed academic components Week 51 – start of year 2 clinical placement
The SCoR Accreditation Scheme Quite rightly the SCoR has issued guidance for all members This has been formalised into the Practice Educator Accreditation Scheme (PEAS) Here it is: https://www.sor.org/career-progression/practice-educators https://www.sor.org/system/files/section/201809/hcp practice educ ation guidance.pdf
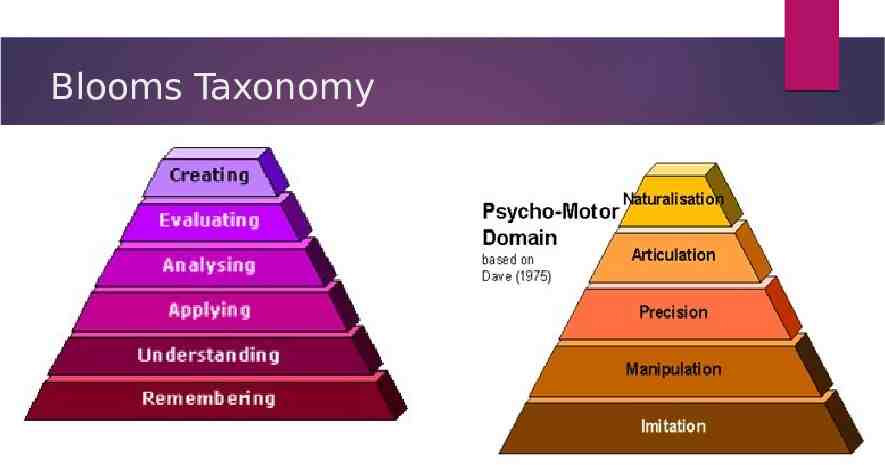
Blooms Taxonomy
Pedagogy – from the greek ped (Child); gogue (Guide) Deep vs Surface Learning (Marten and Säljö (1976)) Learning and Teaching Theories In their study they explored how students would read a text that they were to be questioned on. Some students remembered a list of disjointed facts – essentially ‘skim reading’ to pick out key phrases and passages; other students, however, explored the meaning of the text and sought to understand the author’s position. Strategic learning (Race 2005) where students make a conscious choice about which aspects to learn using a ‘deep’ approach, and which to use a ‘surface’ approach for;
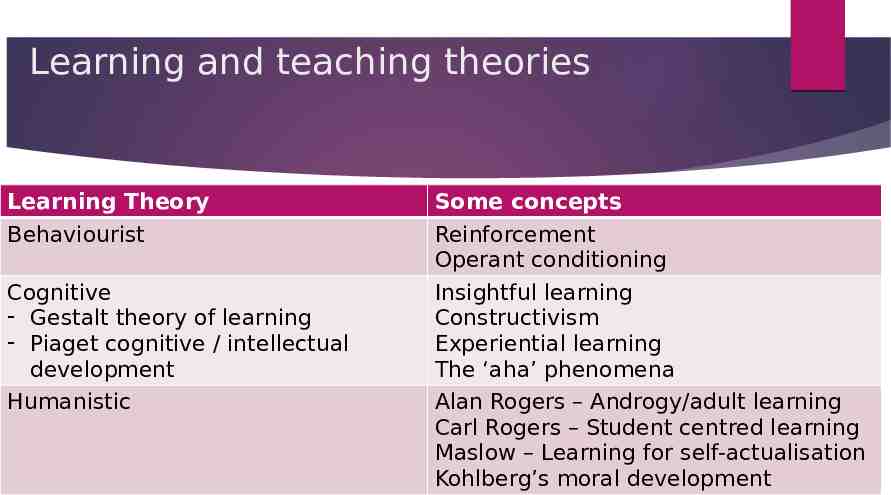
Learning and teaching theories Learning Theory Behaviourist Cognitive - Gestalt theory of learning - Piaget cognitive / intellectual development Humanistic Some concepts Reinforcement Operant conditioning Insightful learning Constructivism Experiential learning The ‘aha’ phenomena Alan Rogers – Androgy/adult learning Carl Rogers – Student centred learning Maslow – Learning for self-actualisation Kohlberg’s moral development
within an educational setting; it is implicit that the teacher is dominant- all instruction is based on guidance from the teacher. In some ways, everything that occurs within a class room is behaviorist. There are some interesting applications of this approach, in instructional corporate presentations or when the response is time critical – during an emergency drill, for example. A widespread extension of the operant conditioning is in the use of feedback, where positive feedback is used to encourage the desired response within a student. Other legacies from this approach are, according to Stewart (2012) include phrases such as ‘learning outcomes’, specifications’, and ‘competencies’. There are some criticisms of this theory, see for example Scales (2008) or Cherry (2014), Stewart (2012) argues that this model in addition to the criticisms of Scales et al are compounded by the emphasis on short term success (measured by learning outcomes) – repetition and rote learning do provide results, but there is no deep understanding. Stewart also argues that, since observable data is measured, there can be no measurement of more abstract concepts, such as thinking. Behaviouris m
Humanism An alternative to operant conditioning is that of Humanism. If operant conditioning results in behaviour bases on the application of consequences, humanism asserts that people act with intentions and values. Rogers (1969) sets out a very clear and alternative to Skinners model. In Rogers’ model 10 principles are outlined regarding learning, as are 10 statements regarding facilitation. Whereas the operant conditioning model almost absolves the teacher of responsibility for student’s failure to engage, in Rogers’s model, the facilitator seems to take personal responsibility for the success or failure of the session, adding in the additional aspect of reflection and acknowledging one’s own limitations.
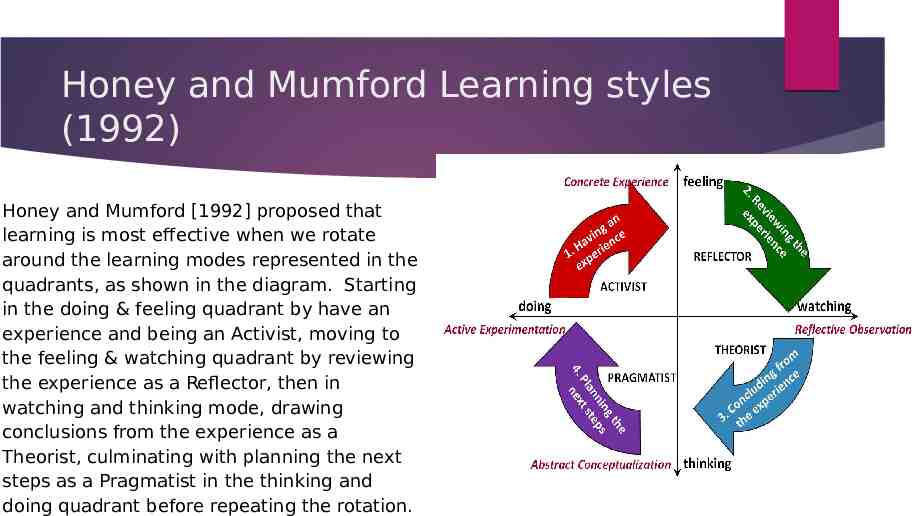
Honey and Mumford Learning styles (1992) Honey and Mumford [1992] proposed that learning is most effective when we rotate around the learning modes represented in the quadrants, as shown in the diagram. Starting in the doing & feeling quadrant by have an experience and being an Activist, moving to the feeling & watching quadrant by reviewing the experience as a Reflector, then in watching and thinking mode, drawing conclusions from the experience as a Theorist, culminating with planning the next steps as a Pragmatist in the thinking and doing quadrant before repeating the rotation.
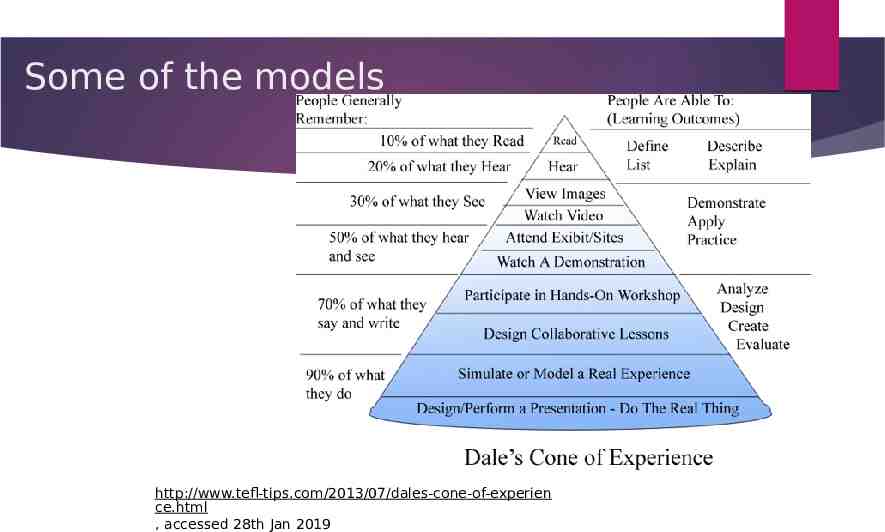
Some of the models http://www.tefl-tips.com/2013/07/dales-cone-of-experien ce.html , accessed 28th Jan 2019
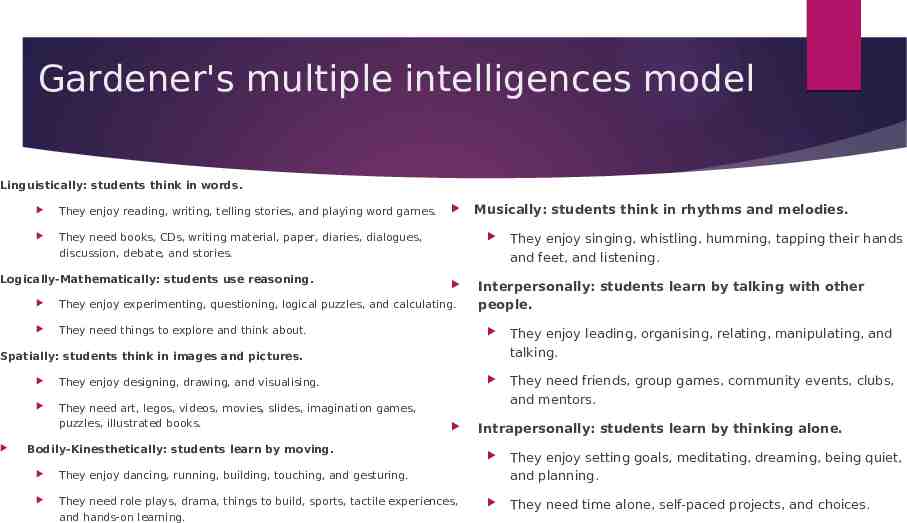
Gardener's multiple intelligences model Linguistically: students think in words. They enjoy reading, writing, telling stories, and playing word games. They need books, CDs, writing material, paper, diaries, dialogues, discussion, debate, and stories. Logically-Mathematically: students use reasoning. Musically: students think in rhythms and melodies. They enjoy experimenting, questioning, logical puzzles, and calculating. They need things to explore and think about. Interpersonally: students learn by talking with other people. They enjoy leading, organising, relating, manipulating, and talking. They need friends, group games, community events, clubs, and mentors. Spatially: students think in images and pictures. They enjoy designing, drawing, and visualising. They need art, legos, videos, movies, slides, imagination games, puzzles, illustrated books. Bodily-Kinesthetically: students learn by moving. They enjoy dancing, running, building, touching, and gesturing. They need role plays, drama, things to build, sports, tactile experiences, and hands-on learning. They enjoy singing, whistling, humming, tapping their hands and feet, and listening. Intrapersonally: students learn by thinking alone. They enjoy setting goals, meditating, dreaming, being quiet, and planning. They need time alone, self-paced projects, and choices.
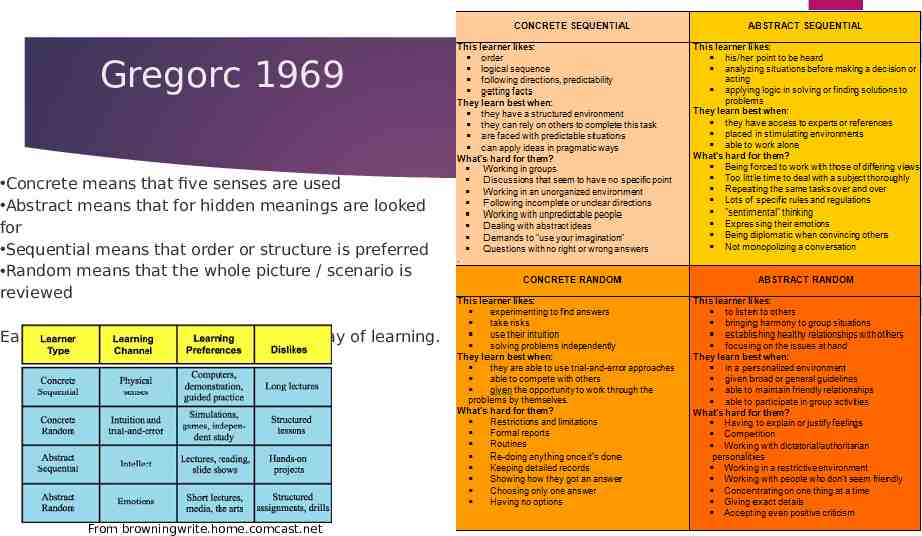
Gregorc 1969 Concrete means that five senses are used Abstract means that for hidden meanings are looked for Sequential means that order or structure is preferred Random means that the whole picture / scenario is reviewed Each learner type preference a certain way of learning. From browningwrite.home.comcast.net
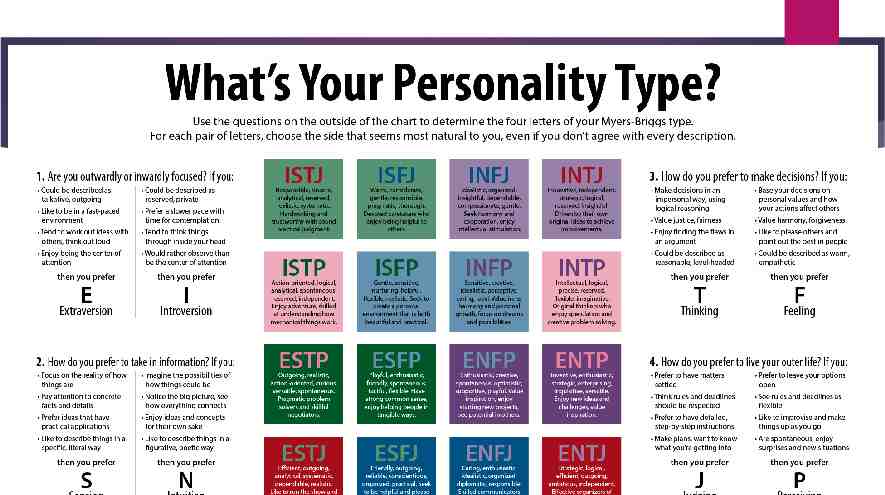
There are other models which you might find useful Other models Meyers-Briggs and Keirsey models – personality types and traits VARK models (Visual, auditory, reading, kinesthetic) Dunn and Dunn (1969) Learning Styles model Grasha and Riechmann (1974) Learning Style scale
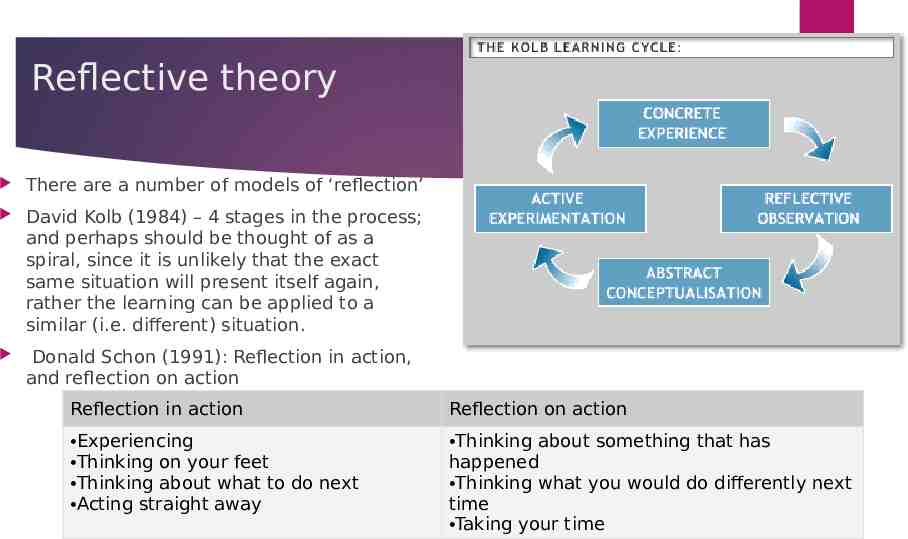
Reflective theory There are a number of models of ‘reflection’ David Kolb (1984) – 4 stages in the process; and perhaps should be thought of as a spiral, since it is unlikely that the exact same situation will present itself again, rather the learning can be applied to a similar (i.e. different) situation. Donald Schon (1991): Reflection in action, and reflection on action Reflection in action Reflection on action Experiencing Thinking on your feet Thinking about what to do next Acting straight away Thinking about something that has happened Thinking what you would do differently next time Taking your time
Reflection in action Schon’s model in practice (an example) You are in a lecture and keep being distracted by thinking about what to have for lunch! You want to get the most from the lecture so need to find a way to help you focus. You decide to start making some notes of the key points. Reflection on action You notice that sometimes after a lecture you can’t remember what was covered. You find out about the lecture topic in advance and write down some questions you want answered. You make notes during the lecture to help you focus. You arrange to go for a coffee after the lecture and talk with your peers about what was presented, to help you understand and form your own opinions. You file your lecture notes and any handouts. You can put these models into practice through reflective writing.
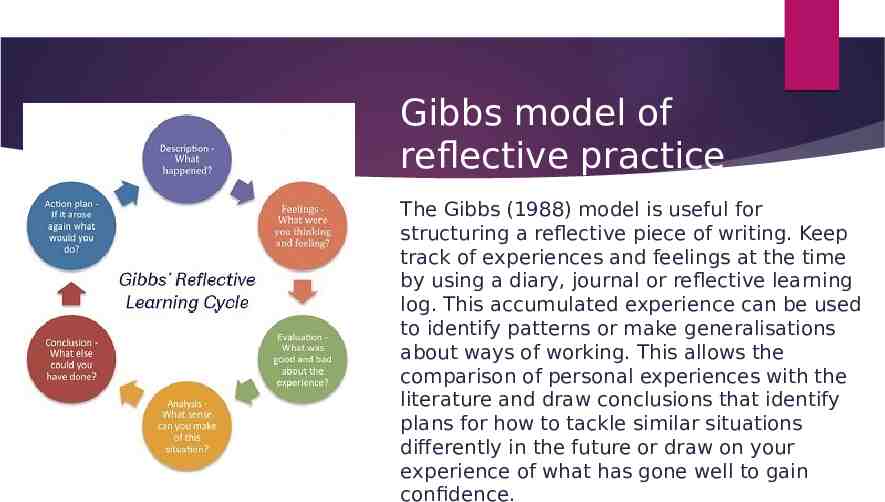
Gibbs model of reflective practice The Gibbs (1988) model is useful for structuring a reflective piece of writing. Keep track of experiences and feelings at the time by using a diary, journal or reflective learning log. This accumulated experience can be used to identify patterns or make generalisations about ways of working. This allows the comparison of personal experiences with the literature and draw conclusions that identify plans for how to tackle similar situations differently in the future or draw on your experience of what has gone well to gain confidence.
Rolfe’s 2001 model Rolfe et al.’s (2001) reflective model is based upon three simple questions: What? So what? Now what? Below is a list of questions that maybe chosen to answer in response to the three elements. What? is the problem/difficulty/ reason for being stuck/reason for feeling bad/reason we don’t get on? was my role in the situation? was I trying to achieve? actions did I take? was the response of others? were the consequences for the student? Myself? Others? feelings did it evoke in the student? Myself? Others? was good/bad about the experience? So what? does this tell me/teach me/imply/mean about me/my class/others/our relationship/my patient’s care/the model of care I am using/my attitudes/my patient’s attitudes? was going through my mind as I acted? did I base my actions on? other knowledge can I bring to the situation? could/should I have done to make it better? is my new understanding of the situation? broader issues arise from the situation? Now what? do I need to do in order to make things better/stop being stuck/improve my teaching/resolve the situation/feel better/get on better/etc., etc.? broader issues need to be considered if this action is to be successful? might be the consequences of this action?
Reflective writing and thinking When is reflective thinking and writing needed? reflecting on practical work/coursework (reflective writing will be assessed – it is for clinical placement assessments). Job applications/interviews: “Tell me about a time when you managed other people and why that was or wasn’t a success”. How? Be objective and be critical of your own actions. Discuss your experiences with others (peers, lecturers, personal tutor) to gain perspective. Compare theories with experiences. Types of reflective writing Stories/narrative: analysis of an event with a beginning, middle and end and a set of characters. Learning journals and logs: reflect on various events at different times. Learning diaries: reflect on events on a frequent basis e.g. daily or weekly. An entry might be on something as specific as a method or technique. Blogs, Twitter, video diaries: good way of ‘selling yourself’ to potential employers and collaborators as a reflective, self-sufficient learner.
Important things to remember with reflective writing Include references - It’s important to remember to include references in your reflective writing. If you choose to use Rolfe et al.’s (2001) model, the easiest place for your references to sit is within the “so what” section. Think about using references to justify why you acted in a particular way – perhaps you read about a particular method that worked in a similar scenario, so you decided that you would also use the same method. You could also easily add in the literature you have read to your “now what” section – perhaps you have read about strategies that you could use to overcome the problems you identified in your reflection and you could tell your reader that you would use them in the future. Keep your writing formal - Many students fall into the trap of writing a “chatty” account of what happened. This is because you are writing a personal account and it’s very easy to write about it informally. Make sure you avoid this and keep your writing academic and formal. Reflective writing and thinking
Constructive Alignment (Bigg’s 1996) What does the student need to be able to do / know at the end of the course (or module / activity)? Can this be expressed as a series of tasks? The teaching and learning activities are designed to achieve the tasks? Implicit in this is the hierarchy of levels of teaching competence, ranging from level 1, where if there is a failure to perform it is the responsibility of the student. At level 3 where concern is on the nature what learning is occurring in the mind of the student – it is not acceptable to blame the student for lack of engagement; Teaching at this level encompasses a wide variety of teaching tools, but if learning is not taking place, then their use is moot. How can the success be measured? Formative – for the student Summative – for the Institution
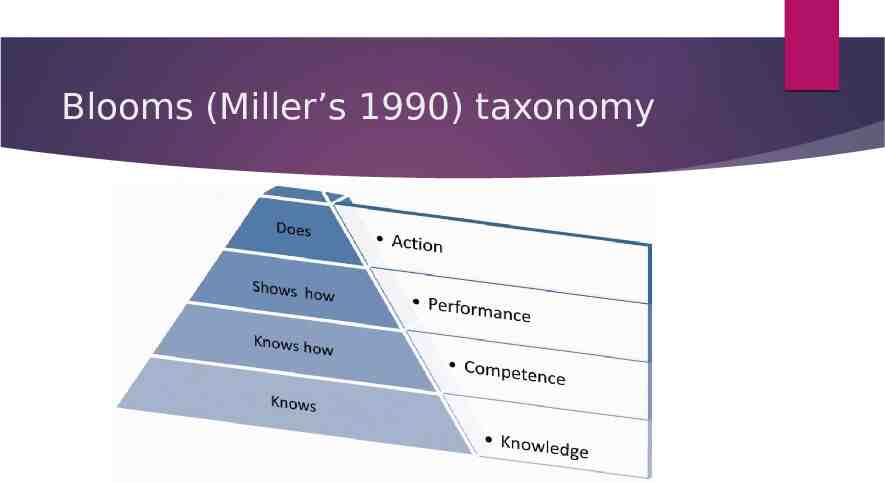
Blooms (Miller’s 1990) taxonomy
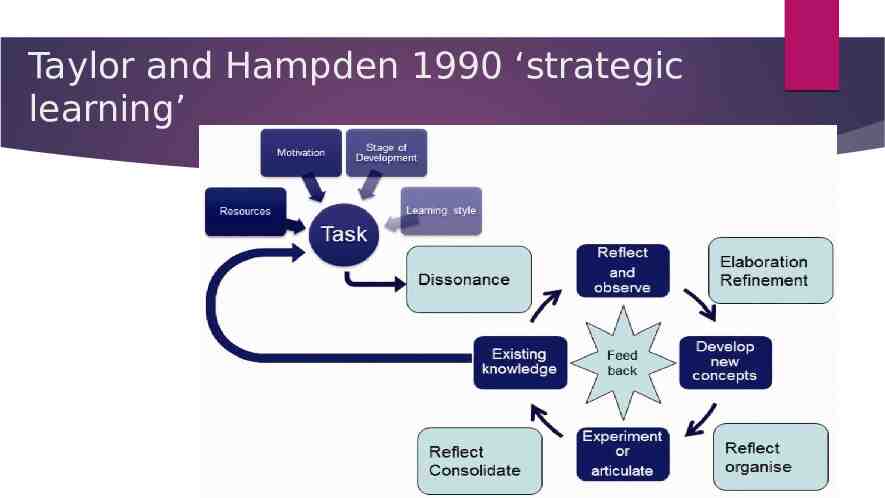
Taylor and Hampden 1990 ‘strategic learning’
3D teaching and learning model –including simulation
What does good practice education look like? A discussion of your experiences
Outline of activities/ session 2 1 2 Criteria for student assessment and DMU documentation Scope, frequency, and content of student conversations Assessing competence When is the student ready? Feedback ‘Failure to fail’ Professional boundaries Disclosure documentation 3 Application to ‘real-life’ situations – impact and progression 4 Professional concerns and fitness to practice When to act How to act
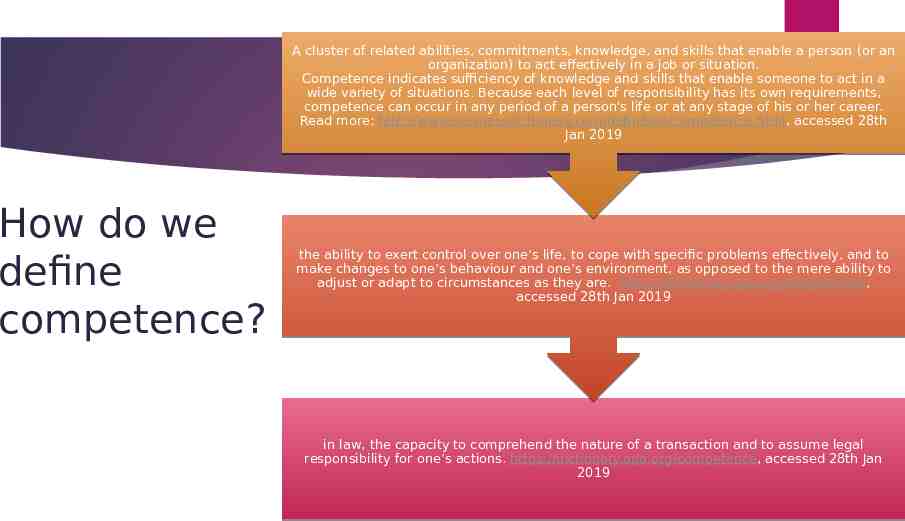
A cluster of related abilities, commitments, knowledge, and skills that enable a person (or an organization) to act effectively in a job or situation. Competence indicates sufficiency of knowledge and skills that enable someone to act in a wide variety of situations. Because each level of responsibility has its own requirements, competence can occur in any period of a person's life or at any stage of his or her career. Read more: http://www.businessdictionary.com/definition/competence.html, accessed 28th Jan 2019 How do we define competence? the ability to exert control over one’s life, to cope with specific problems effectively, and to make changes to one’s behaviour and one’s environment, as opposed to the mere ability to adjust or adapt to circumstances as they are. https://dictionary.apa.org/competence, accessed 28th Jan 2019 in law, the capacity to comprehend the nature of a transaction and to assume legal responsibility for one’s actions. https://dictionary.apa.org/competence, accessed 28th Jan 2019
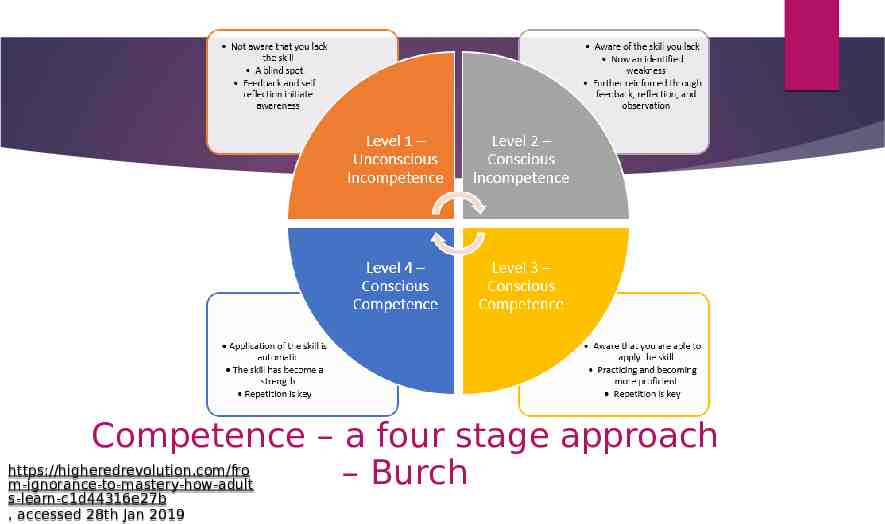
Competence – a four stage approach https://higheredrevolution.com/fro – Burch m-ignorance-to-mastery-how-adult s-learn-c1d44316e27b , accessed 28th Jan 2019
The four stages Conscious incompetence, when people are aware of what they don’t know. New students to clinical practice can be overwhelmed by how much they don’t know or understand, which makes them unproductive. Although they sometimes appear uninterested, the students may, in reality, be frustrated by how much they don’t know, as well as the fact that they may not be being effectively trained and have no idea how to reach out for help. Unconscious incompetence, when people assume that they know something but, in fact, they do not. Ironically, this type of incompetence can set in just as students begin to learn about the role, and the duties and expectations, and how to undertake their role. Training that consists of cramming as much information as possible is not only ineffective in promoting knowledge retention, but it can also trigger a bigger danger: Having completed the training, students (and experienced employees, as well) may incorrectly believe they truly know the information. Instead, they are unconsciously incompetent, which can lead to serious errors, dissatisfied patients, colleagues, and even safety issues. https://higheredrevolution.com/from-ign orance-to-mastery-how-adults-learn-c1d 44316e27b , accessed 28th Jan 2019
The four stages cntd Conscious Competence, a person has acquired the skill they set out to learn and can demonstrate it regularly. Their confidence is improving, but it still takes concentration and intention to perform. In this stage, complacency is the enemy. Practice must continue as mistakes will still be made. In fact, trial and error is necessary to keep learning the skill. Finally, those who have passed through all previous stages reach the fourth and final phase, “Unconscious Competence.” In this stage, application of the skill is automatic, understanding is high, and the skill is now a strength. Those attaining this level of ability must continually seek feedback and guard against regression. Without practice, there is always a risk of falling back to previous stages. Sharing what has been learned with your peers and becoming a mentor is a way to stay sharp and focussed. https://trainingindustry.com/articles/e-lea rning/closing-the-competence-gap-prepa ring-young-professionals-for-the-workforc e/ , accessed 28th Jan 2019 https://higheredrevolution.com/from-ign orance-to-mastery-how-adults-learn-c1d 44316e27b , accessed 28th Jan 2019
Assessment of competence or learning These three domains of assessment are defined as follows: Diagnostic assessment – This is completed when a student begins a specific stage of learning (or placement period) and can initially involve a student self-assessment and a SLOT analysis to assess the strengths, limitations, opportunities and threats relating to the student’s current knowledge, skills and attitudes. It can also include initial observations of the student delivering nursing or health care, discussions on areas of practice, and preliminary questioning, in order to give a baseline on which to build and develop action plans and learning strategies. Formative assessment – This relates to continuous assessment and incorporates regular feedback sessions that are planned throughout the specified time allocated in the learning environment. It gives an opportunity to identify areas of strength and areas that need to be improved, with subsequent action plans developed. It is a method that can be used to monitor progress and provide immediate and ongoing feedback within daily learning experiences. This can also include continuous portfolios of evidence that indicate reflections on learning experiences. Summative assessment – This is usually a more formal process that is designed to assess specific learning outcomes or criteria at a given point in the student’s learning, usually at the end of a period of study (or placement period). This may be an assignment, examination, objective-structured clinical examination, question and answer discussion, observation, portfolio of evidence, or performance indicators including skills https://www.open.edu/openlearn/ocw/mo and competencies. d/oucontent/view.php?id 20113§ion 2 , accessed 28th Jan 2019 slides 34-46
Assessment 1 2 Prior to assessing learning and competence, the student should engage in some form of self-assessment, either by completing a SLOT analysis or by self-assessing against those criteria required for the practice area. Often it can be assumed that the student will be aware of their own capabilities; however, the process of self-assessment will encourage an opportunity to plan learning. You could discuss with the student their: Nevertheless, this process should only be used as one method of assessment in conjunction with others such as direct observation and questioning, which will be needed to confirm current capabilities. Baxter and Norman (2011) suggest that caution is needed when utilising student self-assessment as a method of evidence for competence, as findings from their study recommend this common practice is less than effective and is not an accurate measure of clinical ability when used in isolation. It does however give an insight into how the student perceives their own capabilities and their level of confidence in specific areas of practice. Assessment knowledge base strengths limitations self-perceptions and confidence.
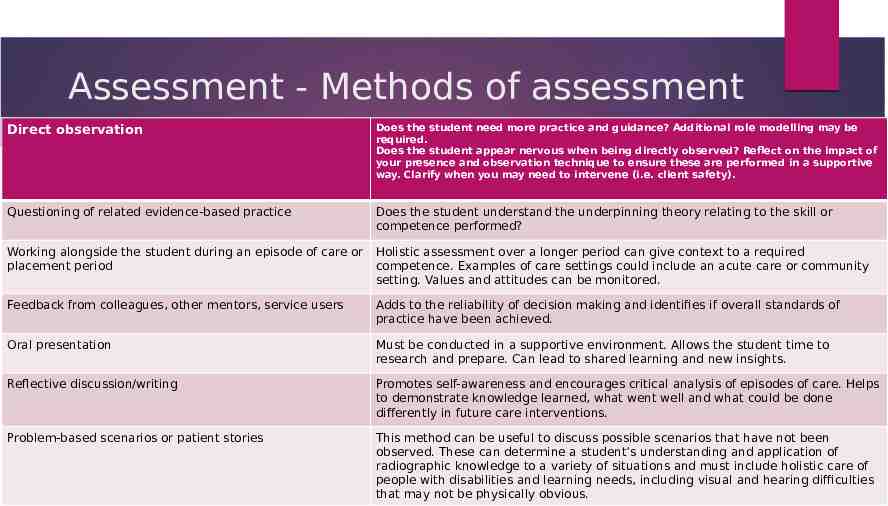
Assessment - Methods of assessment Direct observation Does the student need more practice and guidance? Additional role modelling may be required. Does the student appear nervous when being directly observed? Reflect on the impact of your presence and observation technique to ensure these are performed in a supportive way. Clarify when you may need to intervene (i.e. client safety). Questioning of related evidence-based practice Does the student understand the underpinning theory relating to the skill or competence performed? Working alongside the student during an episode of care or placement period Holistic assessment over a longer period can give context to a required competence. Examples of care settings could include an acute care or community setting. Values and attitudes can be monitored. Feedback from colleagues, other mentors, service users Adds to the reliability of decision making and identifies if overall standards of practice have been achieved. Oral presentation Must be conducted in a supportive environment. Allows the student time to research and prepare. Can lead to shared learning and new insights. Reflective discussion/writing Promotes self-awareness and encourages critical analysis of episodes of care. Helps to demonstrate knowledge learned, what went well and what could be done differently in future care interventions. Problem-based scenarios or patient stories This method can be useful to discuss possible scenarios that have not been observed. These can determine a student’s understanding and application of radiographic knowledge to a variety of situations and must include holistic care of people with disabilities and learning needs, including visual and hearing difficulties that may not be physically obvious.
Assessme nt When completing assessment documentation, you are accountable for the decisions you make. Therefore, you should be detailed, systematic and comprehensive in collating the evidence that is required to inform your judgement. When assessing student competencies, there may be just a signature box to complete within the assessment document, an identified space to write a rationale for a decision or a general comment box following a set of competencies within a specific learning domain. These spaces should always be utilised fully to justify the decision you make. Assessment can be seen to be interpretive and somewhat subjective, so drawing on appropriate evidence when writing your comments can lead to increased confidence in your assessment. This can be discussed openly and honestly with the student. Price (2012) suggests that there should be no surprises for the student when it comes to the final placement interview if effective continual assessment (including regular discussions and constructive feedback) has been implemented. Remember that assessment must be against a set of criteria, and not against another student's performance
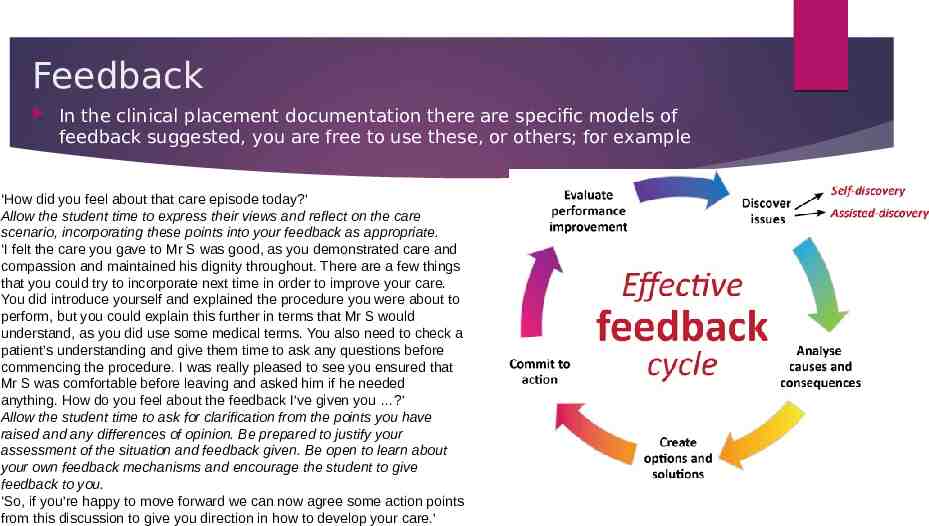
Feedback In the clinical placement documentation there are specific models of feedback suggested, you are free to use these, or others; for example ‘How did you feel about that care episode today?’ Allow the student time to express their views and reflect on the care scenario, incorporating these points into your feedback as appropriate. ‘I felt the care you gave to Mr S was good, as you demonstrated care and compassion and maintained his dignity throughout. There are a few things that you could try to incorporate next time in order to improve your care. You did introduce yourself and explained the procedure you were about to perform, but you could explain this further in terms that Mr S would understand, as you did use some medical terms. You also need to check a patient’s understanding and give them time to ask any questions before commencing the procedure. I was really pleased to see you ensured that Mr S was comfortable before leaving and asked him if he needed anything. How do you feel about the feedback I’ve given you ?’ Allow the student time to ask for clarification from the points you have raised and any differences of opinion. Be prepared to justify your assessment of the situation and feedback given. Be open to learn about your own feedback mechanisms and encourage the student to give feedback to you. ‘So, if you’re happy to move forward we can now agree some action points from this discussion to give you direction in how to develop your care.’
Support for the failing student We have looked specifically at the processes of assessment and how to deliver constructive feedback in the practice setting. You also explored various methods of assessment and considered feedback strategies. The aim now is to discuss the strategies and skills that will help you to identify the student who is either failing or has failed and provide the appropriate opportunities and support for them to meet the required competencies in order to successfully complete their placement. Most students of radiography achieve their required competencies in practice. However, there are a few whose performance may be considered weak and who have trouble in meeting the required standards. It will be necessary to provide extra support and supervision for these students. Duffy’s (2003) study is a significant piece of research that has contributed to the literature on reasons why mentors lack confidence in failing students, with more recent research replicating many of Duffy’s original findings. For example, a later study by Gainsbury (2010) found that a quarter of interviewees felt unconfident in managing students’ performance. Further evidence (Brown et al., 2012; Heaslip and Scammell, 2012) suggests that mentors find this aspect of their role most challenging and are reluctant to fail students when they do not perform as expected. This may occur because the student may display behaviours that can be hard to identify (Duffy, 2004; Skingley et al., 2007; Black et al., 2014). In this context, as a mentor you need to work closely with students to provide support or opportunities as required
Duffy and Hardicre (2007b) and Black et al. (2013) list a range of issues that suggest why learners fail to engage with practice. You may have noted similar issues from your reflection and discussion with others. These include: Recognition of the failing student a lack of insight, poor self-awareness and unresponsiveness to feedback a lack of interest, motivation, enthusiasm or commitment – not asking questions, poor communication or interpersonal/interactional skills – insensitive interaction with patients frequently late or absent, exhibit poor preparation and organisational skills preoccupation with personal issues – poor health, withdrawn, sad and tired poor professional behaviour/boundary issues, either overconfident or underconfident lack of theoretical knowledge and skill, and provides limited evidence to support their learning avoidance of working with the mentor and changing shifts unsafe practice and poor judgement. It is important to raise and document your concerns regarding underperformance at the earliest opportunity and not to ignore problems as they occur. Evidence suggests that if you take time to explore the issues early and put an action plan into place, this may enable the learner to rescue what may originally be considered a failing situation (Duffy and Hardicre, 2007a).
Breakin g bad news – failing a student Breaking bad news is never an easy option, so informing a student near the end of their programme of study that they have failed their placement will naturally upset the individual. Walsh (2014) explains how students may react to the outcome of assessment with a feelings which may include: denial – they respond with disbelief and shock to a failed assessment betrayal – they may feel hurt that their friend has failed them (some students interpret the supportive mentorship relationship as a close friendship rather than a professional one) sadness – some will cry, which can be upsetting for the mentor relief – some students may be relieved and willing to accept a failed assessment. In some instance's failure can have a positive outcome. Support is crucial for students who perceive this as a stressful experience. An opportunity should be provided for them to repeat the experience when appropriate, and to have access to a range of support services from the HEI, linked lecturers, module leaders, counselling and student union processes. It will depend though on the University policy for repeating clinical placement / assessment
Breaking bad news cntd This can be an equally stressful experience for the mentor, who will require support. Managing the process of underachieving or failing students must be made with confidence (Brown et al., 2012). A decision to fail a student nearing the end of the programme can be a challenge, because the underperformance should have been addressed earlier. your decision could cause tensions within the team or the organisation if it is perceived that some of the mentors assessing students on their previous placements did not fulfil their assessment obligations. However, failing to fail students can have serious consequences for the service users, who may be put at risk. Unfortunately some students will attempt to use coercive techniques to manipulate a mentor/assessment decision, Hunt et al (2016) outlines these, and some techniques to avoid them: Ingratiators – deliberately charming, indulging, or emotionally exploitative Diverters – students attempt to distract or redirect the mentors focus by exaggerating the effects of external processes Disparagers – students whom challenge the mentor in belittling, denigrating, or professionally harmful ways; accusing the mentor of bullying, harassment, and intimidation. Aggressors – students whom demonstrate open hostility towards their mentor after receiving negative feedback or bad news, either verbally or physically; or via third party. Mentors require support and guidance when they fail students, because they must deliver difficult messages to the underperforming student. They need to develop confidence and must be clear about the roles and responsibilities in making these decisions.
Breakin g bad news cntd. Mentors need to familiarise themselves with students’ documentation and assessment regulations and must keep accurate records to support and justify their decisions on whether a student is competent or not. They need to demonstrate that they have provided regular feedback and kept a record of this while mentoring students (Walsh, 2014). They can then make valid assessments on whether a student is competent or not. In practice, the consequences of not failing students are that we fail in our duty of care to protect the safety of those whom we serve.
Your role in evaluating practice learning in your area will include some involvement with educational audit. This is a process that is required by the regulating body (the HCPC) to assure standards are met in relation to student learning in practice. Education providers are responsible for organising and completing bi-annual audits of all placement areas used for student clinical placements. This is done in partnership with placement providers and will involve link tutors, clinical education leads and facilitators, healthcare managers, practice teachers, mentors, and students. Each education provider will have its own format, criteria, and audit process, so it is important that you are familiar with these and have sight of the most current audit for your practice area, what are the areas of good practice, and what needs improving. In some areas of the UK, higher education institutes will work together to share educational audit assessment. Education audit
You may have been involved in peer review as part of educational processes relating to assessment, or as part of an appraisal process such as 360-degree feedback from colleagues. There are more tools available on the NHS Leadership Academy website You may also relate peer review to the role of a ‘critical friend’ who has the expertise to give constructive feedback on your performance. As part of your continuing development as a mentor, it is important to seek feedback on your own mentorship practices and also contribute to mentor colleagues’ development. This can be both informal and formal depending on your practice areas’ guidance and requirements. Peer review However, the process of peer review can encourage and support mentors in continuous improvement. Peer review should involve those of the same status or role, which in this context are your fellow mentors. Peer review should not be seen as a ‘pass’ or ‘fail’ activity but should be seen as providing constructive feedback on performance and discussing areas for improvement. This is similar to the constructive feedback processes discussed earlier. Peer review, when conducted effectively, also helps to build confidence in the person being ‘reviewed’ and ultimately embeds a culture of mentorship excellence in the ‘reviewer’ feeding back to colleagues.
Scope, frequency and content of student discussions Within the CPAD there is a template for student discussions, and a model of an action plan pro-forma. We suggest a weekly meeting with the student to review progress against aims for the particular week. Each month academic link tutors will visit the students on clinical placement and seek to have a conversation with clinical staff involved with student education. There will, in addition, meetings with the both the student and practice education team. The structure of these discussions is intended to be a constructive positive experience for all concerned, and clinical staff are encouraged to reflect on the line, style, and phraseology used when exploring students understanding of a particular area, issue, or technique. Staff should also be mindful of the stage of student training, and their academic course content.
Scope, frequency and content of student discussions We would consider it good practice, during the initial meeting, that the scope and nature of discussions is outlined. This could include an outline of expectations from both parties (i.e. the student and practice educator) It may require a formal 'learning contract' It should also state what the limits of confidentiality are including disclosure Clinical staff should have a clear view of the processes of assessment, and of the fitness to practice / concerns procedures Clinical staff should have confidence in the processes and procedures for student discipline within the academic setting
Effective questioning? Underpinning all the assessment methods explored previously is effective questioning, which helps to: understand the students’ thought processes assess students’ critical thinking skills and decision-making capabilities clarify the processes and actions observed ascertain understanding of the various components of a care intervention encourage further reflection. Carlson et al. (2009) suggest that questioning is the most commonly used form of student–mentor interaction, should be planned carefully in relation to the student’s stage of learning and should not be interrogative or judgmental. Ness (2010, p. 42) identifies key points below when asking students in practice questions to assess their learning: Do my questions relate to the students learning outcomes? Are my questions clear? Do my questions help the student link theory to practice? Are my questions at the appropriate academic level for the student? Are my questions seen as threatening? Am I asking too many questions at once? Am I asking questions in an appropriate place? Am I asking questions at an appropriate time? Do I listen to the student’s response?
The paperwork See the attached handouts! A discussion about the paperwork
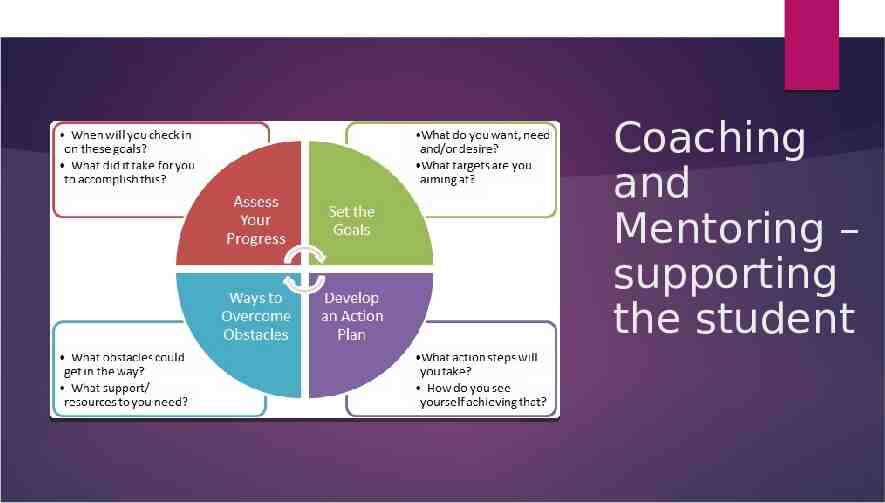
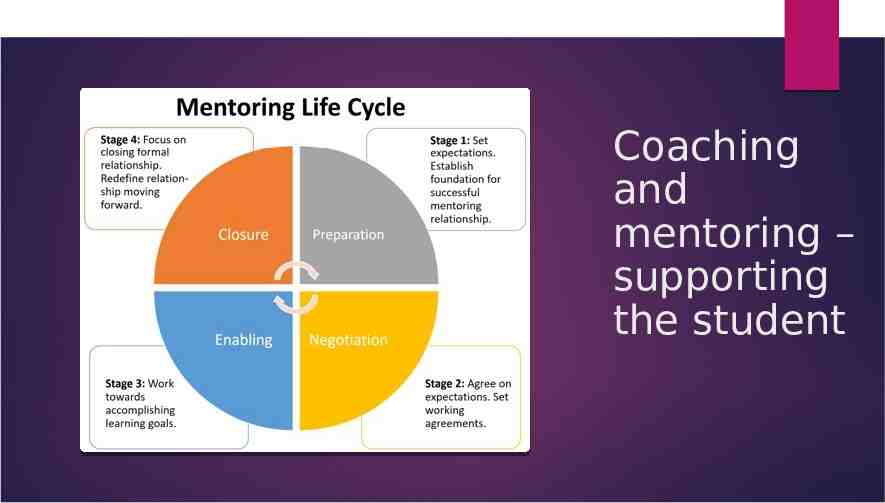
Coaching and Mentoring – supporting the student
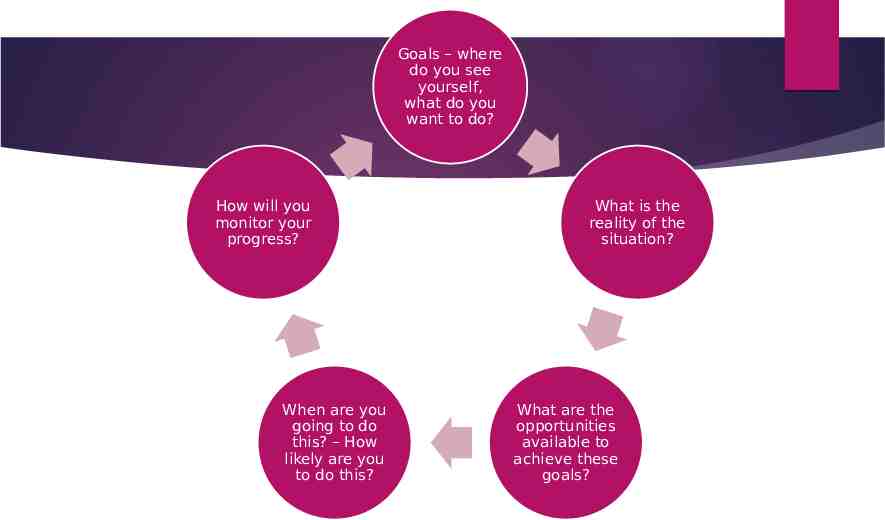
Goals – where do you see yourself, what do you want to do? How will you monitor your progress? When are you going to do this? – How likely are you to do this? What is the reality of the situation? What are the opportunities available to achieve these goals?
Coaching and mentoring Coaching: Coaching: Is Is performance performance driven. driven. The The purpose purpose of of coaching coaching is is to to improve improve the the individual's performance on the individual's performance on the job. job. This This involves involves either either enhancing enhancing current current skills skills or or acquiring acquiring new new skills. skills. Once Once the the coachee coachee successfully successfully acquires acquires the the skills, skills, the the coach coach is is no no longer longer needed. needed. Is focus is Is task task oriented. oriented. The The focus is on on concrete issues, such as managing concrete issues, such as managing more more effectively, effectively, speaking speaking more more articulately, and learning how articulately, and learning how to to think think strategically. strategically. This This requires requires a a content expert (coach) who can content expert (coach) who can teach teach the the coachee coachee how how to to develop develop these skills. these skills. Is Is short short term. term. A A coach coach can can successfully be involved with successfully be involved with a a coachee coachee for for a a short short period period of of time, time, maybe maybe even even just just a a few few sessions. sessions. The coaching lasts for The coaching lasts for as as long long as as is is needed, depending on the purpose needed, depending on the purpose of of the the coaching coaching relationship. relationship. does does not not require require design. design. Coaching Coaching can be conducted can be conducted almost almost immediately immediately on on any any given given topic. topic. In In coaching, coaching, the the coachee's coachee's immediate immediate manager manager is is a a critical critical partner. She or he often provides partner. She or he often provides the the coach coach with with feedback feedback on on areas areas in in which his or her employee needs which his or her employee needs coaching. coaching. This This coach coach uses uses this this information to guide the coaching information to guide the coaching process process
Coaching and mentoring – supporting the student
Coaching and mentoring Mentoring: Mentoring: Is Is relationship relationship oriented. oriented. It It seeks seeks to to provide a safe environment provide a safe environment where where the the mentee mentee shares shares whatever whatever issues issues affect affect their their professional professional and and personal personal success. success. Although Although specific specific learning learning goals goals or or competencies competencies may may be be used used as as a a basis basis for for creating creating the the relationship, relationship, its its focus focus goes goes beyond beyond these these areas areas to to include include things, things, such such as as work/life work/life balance, balance, self-confidence, self-confidence, self-perception, self-perception, and and how how the the personal personal influences the professional. influences the professional. Is Is always always long long term. term. Mentoring, Mentoring, to to be be successful, requires time in which successful, requires time in which both both partners partners can can learn learn about about one one another another and and build build a a climate climate of of trust trust that that creates creates an an environment environment in in which which the the mentee mentee can can feel feel secure secure in in sharing sharing the the real real issues issues that that impact impact their their success. success. Successful Successful mentoring mentoring relationships relationships last last nine nine months months to to a a year. year. Is Is development development driven.Its driven.Its purpose purpose is is to to develop develop the the individual individual not not only only for for the the current current job, job, but but also also for for the the future. future. This This distinction distinction differentiates differentiates the the role role of of the the immediate immediate manager manager and and that that of of the the mentor. mentor. It It also also reduces reduces the the possibility possibility of of creating creating conflict conflict between between the the employee's employee's manager manager and and the the mentor. mentor. requires requires a a design design phase phase in in order order to to determine the strategic purpose determine the strategic purpose for for mentoring, mentoring, the the focus focus areas areas of of the the relationship, the specific mentoring relationship, the specific mentoring models, models, and and the the specific specific components components that that will guide the relationship, will guide the relationship, especially especially the the matching matching process. process. the the immediate immediate manager manager is is indirectly indirectly involved. Although they involved. Although they may may offer offer suggestions suggestions to to the the employee employee on on how how to to best best use use the the mentoring mentoring experience experience ,, the the manager manager has has no no link link to the mentor, and they do to the mentor, and they do not not communicate communicate at at all all during during the the mentoring mentoring relationship. This helps maintain relationship. This helps maintain the the mentoring mentoring relationship's relationship's integrity. integrity.
Learning Outcomes: are you/ do you? 1 By the end of these sessions 2 comfortable with the educational terminology used 3 4 Have a deeper understanding of your role and responsibilities with regards to student placement experiences Know when, to whom, and how to escalate concerns
Some reading on this and other topics Benner, P. (2000) From Novice to Expert: Excellence and Power in Clinical Nursing Practice, Upper Saddle River, NJ, Prentice Hall. Cant, R., McKenna, L. and Cooper, S. (2013) ‘Assessing preregistration nursing students’ clinical competence: a systematic review of objective measures’, International Journal of Nursing Practice, vol. 19, no. 2, pp. 163–76. Gopee, N. (2011) Mentoring and Supervision in Healthcare, London, Sage. Joghin, G. (ed.) (2009) Assessment, Learning and Judgment in Higher Education, Wollangong, Australia, Springer. Hunt l., McGee P., Gutteridge R., Hughes M (20160 manipulating mentors'assessemnt decisions: Do underperforming student nurses use coercive strategies to influence mentors' assessment decisions? Nurse education in Practice 20 (2016) 154-162 Rolfe, G., Freshwater, D., Jasper, M. (2001) Critical reflection in nursing and the helping professions: a user’s guide. Basingstoke: Palgrave Macmillan.
Any final thoughts or questions?
References Duffy, K. (2013) ‘Providing constructive feedback to students during mentoring’, Nursing Standard, vol. 27, no. 31, pp. 50–56. Anderson, L. (2011) ‘A learning resource for developing effective mentorship in practice’, Nursing Standard, vol. 25, no. 51, pp. 48– 56. Faculty of HealthUOP’s channel [YouTube user] (2010) ‘Describe yourself on a placement’ (online), YouTube, 2 March. Available at https://www.youtube.com/ watch?v job59GG2bR4 (Accessed 24 February 2015). Aston, L. and Hallam, P. (2014) Successful Mentoring in Nursing, 2nd edn, London, Sage. Baxter, P. and Norman, G. (2011) ‘Self-assessment or self-deception? A lack of association between nursing students’ self-assessment and performance’, Journal of Advanced Nursing, vol. 67, pp. 2406–13 . Brown, L. (2012) ‘What influences mentors to pass or fail students’, Nursing Management, vol. 19, no. 5, pp. 16–21. Brugnolli, A., Perli, S., Viviani, D. and Saiani, L. (2011) ‘Nursing students’ perceptions of tutorial strategies during clinical learning instruction: a descriptive study’, Nurse Education Today, vol. 31, no. 2, pp. 152–6. Carlson, E., Wann-Hansson, C. and Pilhammar, E. (2009) ‘Teaching during clinical practice: strategies and techniques used by preceptors in nursing education’, Nurse Education Today, vol. 29, no. 5, pp. 522–6. Casey, D. and Clark, L. (2014) ‘Involving patients in the assessment of nursing students’, Nursing Standard, vol. 28, no. 47, pp. 37–41. Clynes, M.P. and Rafferty, S.E. (2008) ‘Feedback: an essential element of student learning in clinical practice’, Nurse Education in Practice, vol. 8, no. 6, pp. 405–11. Dohrenwend, A. (2002) ‘Serving up the feedback sandwich’, Family Practice Management, vol. 9, no. 10, pp. 43–9. Fahy, A., Tuohy, D., McNamara, M.C., Butler, M.P., Cassidy, I. and Bradshaw, C. (2011) ‘Evaluating clinical competence assessment’, Nursing Standard, vol. 25, no. 50, pp. 42–8. Jerome, P.J. (1995) Coaching through Effective Feedback, London, Kogan Page. Murray, C., Rosen, L. and Staniland, K. (eds) (2010) The Nurse Mentor and Reviewer Update Book, Maidenhead, Open University Press. Ness, V. (2010) ‘Supporting and mentoring nursing students in practice’, Nursing Standard, vol. 25, no. 1, pp. 41–6. Nursing and Midwifery Council (NMC) (2008) Standards to Support Learning and Assessment in Practice: NMC Standards for Mentors, Practice Teachers and Teachers, London, NMC. Nursing and Midwifery Council NMC (2010) Standards for Pre-registration Nursing Education, London, NMC. Available at http://standards.nmc-uk.org/ PublishedDocuments/ Standards%20for%20pre-reg istration%20nursing%20education%2016082010.pdf (Accessed 24 February 2015). Price, B. (2012) ‘Key principles in assessing students’ practice-based learning’, Nursing Standard, vol. 26, no. 49, pp. 49–55. Quinn, F.M. and Hughes, S.J. (2007) Quinn’s Principles and Practice of Nurse Education, 5th edn, Andover, Cengage Learning.