PSYCHOLOGICAL TESTING Esther Schwartz, PhD & David Trotter, PhD
25 Slides456.91 KB
PSYCHOLOGICAL TESTING Esther Schwartz, PhD & David Trotter, PhD
OBJECTIVES 1. Provide essential background information on psychological assessment domains and common instruments 2. Help you be informed consumers of psychological data in your future medical practice 3. Present material that will be covered in the USMLE Step 1
OVERVIEW Psychological tests are used to assess intelligence, achievement, personality, and psychopathology. Psychological assessment is typically driven by a particular problem or referral question. The purpose of assessment is to answer particular questions related to an individual’s intellectual, psychological, emotional-behavioral, or psychosocial functioning, or some combination of these domains. Referrals generated in the medical setting may include 1: Evaluate child’s defiant behavior and poor academic performance. Patient’s depression screen is positive. Patient has a complicated psychiatric history. Evaluate. Determine psychological readiness to undergo surgical procedure (e.g., organ transplants, bariatric, amputation) ALTMAIER & TALLMAN, 2013
TESTING IN CONTEXT Psychological testing is one component of psychological assessment Gather information from the patient (clinical interview/behavioral observations) Obtain collateral information (parent, school) Administer psychological test instruments Test battery will look at functioning in a number of different functional areas. Use tests that have been standardized for a specific population within a specific context so scores are reliable and valid in describing abilities. Interpret the results Report will test combine data with the collateral and interview data This conceptualization is summarized, a diagnosis or a diagnostic rule-out is offered Recommendations are made
LIMITATIONS Bias Psychologist may selectively attend to behaviors that are consistent with their expectations or theoretical orientation (confirmatory bias) Preference and availability of certain instruments Patient factors Motivation Effort on a continuum (positive impression management, optimal effort, passively cooperative, suboptimal effort, negative impression management, malingering) Comfort with the testing situation Assessment of diverse populations Culture, ethnicity, race, primary language, SES, level of education are variables that that influence test results. Validity of test results may be attenuated when instruments are used inappropriately cross-culturally. Stereotype threat2 STEELE & ARONSON, 1995
INTELLIGENCE
INTELLIGENCE Intelligence is defined as the ability to understand abstract concepts; reason; assimilate, recall, analyze, and organize information; and meet the special needs of new situations. Is intelligence a single general ability or are there several distinct kinds of intelligence? Spearman: General cognitive ability (g factor) Cattell Fluid Intelligence: capacity to acquire new knowledge and solve new problems, and is partially determined by biological and genetic factors. Crystallized intelligence: knowledge and learning gained over one’s lifetime through an interaction between fluid intelligence and environment (i.e., culture, education)
INTELLIGENCE IQ is determined to a large extent by genetics. Substantial heritability of g has been documented in dozens of family, twin, and adoption studies, with estimates varying from 40 to 80%. In 34 twin studies with a total of 4672 pairs of MZ twins, the average MZ correlation is 0.86, indicating that the identical twins are nearly as similar as the same person tested twice (test-retest correlation for g is about 0.90). In contrast, the average DZ correlation is 0.60 in 41 studies, with a total of 5546 pairs of DZ twins.3 Heritability of g seems to increase with age. Genetic factors account for approximately 50% of population–level variation in intelligence by the end of the first decade of life. This proportion increases to 70% by late adolescence.4 However, poor nutrition and illness during development can negatively affect IQ. IQ is relatively stable throughout life. G is one of the most reliable, valid, and stable behavioral traits. In the absence of brain pathology, an individual’s IQ is essentially the same in old age as in childhood. BOUCHARD & MCGUE, 1981; HAWORTH, 2010
INTELLIGENCE AND MENTAL AGE Seminal work by Binet and colleagues (Simon) in the early 1900s. Binet’s fundamental assumption was that intellectual capacities in children increased with age on average, so that older children were expected to perform better than younger children on the same items. Chronological Age (CA) is the person’s actual age in years. Mental Age (MA), as defined by Alfred Binet, reflects a person’s level of intellectual functioning. A student with a mental age of 10 performed as well as the average 10-year old in the normative sample. IQ is the ratio of MA to CA multiplied by 100 (i.e., IQ MA/CA x 100) An IQ of 100 means that the person’s mental and chronological ages are equivalent. The highest CA used to determine IQ is 15 years.
QUESTION A child is tested and found to have a mental age of 12 years. The child’s chronological age is 10 years. What is the IQ of this child? (A) 40 (B) 60 (C) 80 (D) 100 (E) 120 Answer: IQ MA/CA x 100 12/10 x 100 120
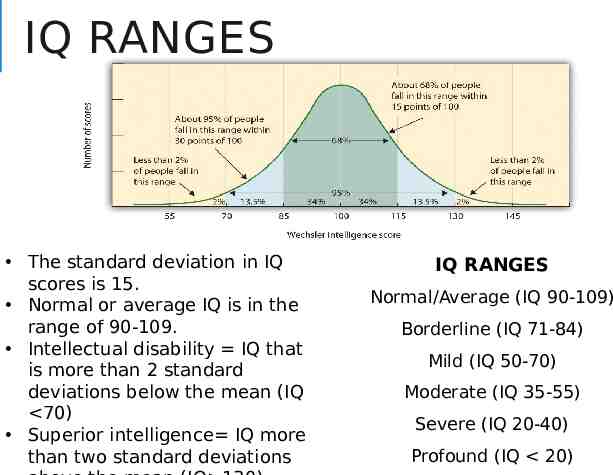
IQ RANGES The standard deviation in IQ scores is 15. Normal or average IQ is in the range of 90-109. Intellectual disability IQ that is more than 2 standard deviations below the mean (IQ 70) Superior intelligence IQ more than two standard deviations IQ RANGES Normal/Average (IQ 90-109) Borderline (IQ 71-84) Mild (IQ 50-70) Moderate (IQ 35-55) Severe (IQ 20-40) Profound (IQ 20)
QUESTION A 12-year old child who is having difficulty in school is given an intelligence test. The test determines that the child is functioning mentally at the level of an 8-year old child. What category of intellectual function bests describes this child? (A) Severely intellectually disabled (B) Moderately intellectually disabled (C) Mildly intellectually disabled (D) Borderline (E) Normal or average Answer: IQ MA/CA x 100 8/12 x 100 66 Mild Intellectual disability (IQ 5070)
COMMON INTELLIGENCE TESTS The Wechsler Adult Intelligence Scale-Fourth Edition (WAISIV) is the most commonly used intelligence test for adults and older adolescents (16-90 years of age). Standardization sample for WAIS-IV (N 2,200) was selected according to 2005 U.S. Census Data and was stratified according to age, sex, race/ethnicity, geographic region, and educational level. The Wechsler Intelligence Scale for Children (WISC) is used to test intelligence in children 6-16 ½ years of age. The Wechsler Preschool and Primary Scale of Intelligence (WPPSI) is used to test intelligence in children 4-6 ½ years of age. Stanford-Binet Intelligence Scales Non-verbal tests include: Leiter International Performance, Universal Nonverbal Intelligence Test, Naglieri Nonverbal Ability Test IQ test scores are less reliable for populations that approach the extreme ends of the spectrum of ability.
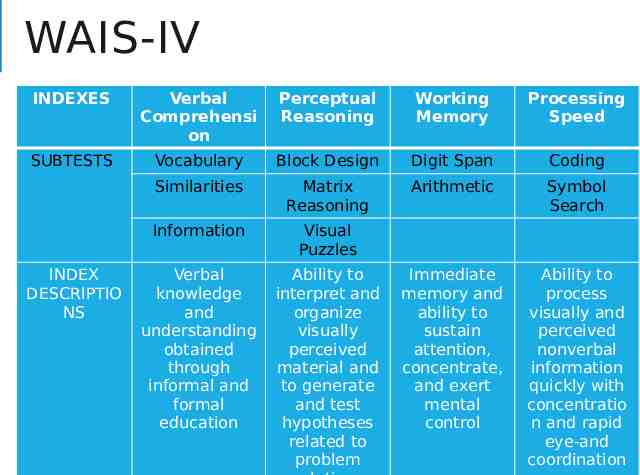
WAIS-IV INDEXES Verbal Comprehensi on Perceptual Reasoning Working Memory Processing Speed SUBTESTS Vocabulary Block Design Digit Span Coding Similarities Matrix Reasoning Arithmetic Symbol Search Information Visual Puzzles Verbal knowledge and understanding obtained through informal and formal education Ability to interpret and organize visually perceived material and to generate and test hypotheses related to problem Immediate memory and ability to sustain attention, concentrate, and exert mental control Ability to process visually and perceived nonverbal information quickly with concentratio n and rapid eye-and coordination INDEX DESCRIPTIO NS
INTELLECTUAL DISABILITY Intellectual Disability (Intellectual Disability Disorder) 3 criteria: Deficits in intellectual functions (e.g., reasoning, planning, judgment) confirmed by clinical assessment and standardized intelligence testing. Deficits in adaptive functioning (e.g., communication, social participating, independent living) Onset of intellectual and adaptive deficits during the developmental period. Specify Mild, Moderate, Severe, Profound Specifiers of severity are based on adaptive functioning NOT IQ scores, because it is adaptive functioning that determines the level of supports required. Of those with ID, 85% have mild impairment, 10% have moderate, and 5% have severe to profound impairments. Prevalence of ID Worldwide prevalence: 1% (estimates vary between countries, income levels, etc) ID is approximately 5 times higher for males than for females.
ADAPTIVE BEHAVIOR ASSESSMENT Assessment of adaptive behavior is necessary for diagnosis of intellectual disability. Provides information about a person’s strengths and weaknesses that can inform educational and intervention efforts. Among the very large number of adaptive behavior scales on the market, very few have adequate norms and reliability to diagnose intellectual disability in people with IQs in the 70 range. Vineland Adaptive Behavior Scales-Survey Form Scales of Independent Behavior
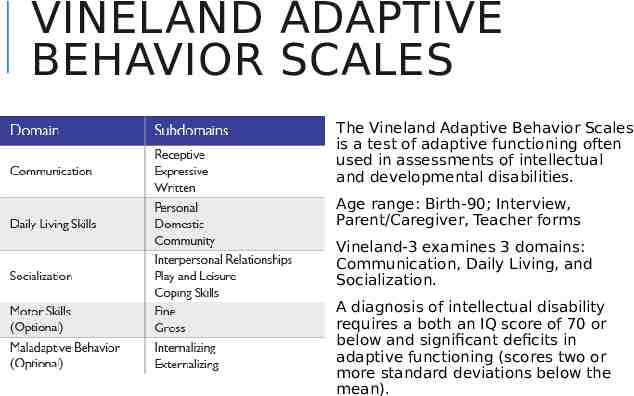
VINELAND ADAPTIVE BEHAVIOR SCALES The Vineland Adaptive Behavior Scales is a test of adaptive functioning often used in assessments of intellectual and developmental disabilities. Age range: Birth-90; Interview, Parent/Caregiver, Teacher forms Vineland-3 examines 3 domains: Communication, Daily Living, and Socialization. A diagnosis of intellectual disability requires a both an IQ score of 70 or below and significant deficits in adaptive functioning (scores two or more standard deviations below the mean).
ACHIEVEMENT “I dreamed I was being chased by a giant standardized test.”
ACHIEVEMENT TESTS Achievement tests are used to assess academic achievement (e.g., evaluate how well an individual has mastered specific subject areas, such as reading and mathematics). Achievement tests include the Scholastic Aptitude Test (SAT), Medical College Admission Test (MCAT), and the United States Licensing Examination (USMLE). The Wide Range Achievement Test (WRAT), which is often used clinically, evaluates arithmetic, reading, and spelling skills. Achievement tests often used by school systems include the California, Iowa, Stanford, and Peabody Achievement Tests.
LEARNING DISORDERS Ability-achievement Discrepancy Traditionally, learning disability was defined as significantly lower academic achievement relative to one’s measured intellectual ability. 6 But, this assumes that factors that negatively affect academic achievement scores do not influence scores on IQ tests. Specific learning disorders Difficulties of learning and using specific academic skills in certain learning domains (i.e., word reading, reading comprehension, spelling, written expression, number sense, mathematical reasoning) that are substantially below individual's chronological age, and cause significant interference with academic or occupational performance. Although intellectual assessment has been the core of psychological assessment for LD for decades, it is no longer required for a DSM- 5 diagnosis of SLD, except when Intellectual Disabilities are suspected. APA, 2000
PSYCHOPATHOLOGY In medical settings the most common psychopathology you will encounter will relate to symptoms of depression, anxiety, and substance abuse. Evaluation of patients with emotional symptoms involves: Psychiatric history Includes mental illness, drug and alcohol use, sexual activity, current living situation, and sources of stress. Mental Status Exam Data from personality testing and symptom inventories
DEPRESSION SCALES Major depression and symptoms of depression are common among patients presenting in medical settings. Pearson et al. (1999) demonstrated that 20% of patients identified as high utilizers of medical care experienced major depression or major depression in partial remission. Objective rating scales of depression that are commonly used include the Hamilton, Raskin, Zung, and Beck. In the Hamilton and Raskin scales, an examiner rates the patient. In the Zung and Beck scales the patient rates self.
ITEMS IN THE BECK DEPRESSION INVENTORY-II BDI-II Most common screening tool to identify severity of depression in medical settings. 21-item self-report scale of depressive symptoms. Acceptable psychometric qualities among medical populations and minority populations BDI-II assesses: Sadness Dislike of self Pessimism Self-blame Sense of failure Selfcriticalness Loss of pleasure Suicidal ideation Guilt Episodes of crying Expectation of punishment Agitation Loss of interest Appetite changes Indecisivenes s Concentratio n problems Worthlessnes s Fatigue Loss of energy Sleep changes Low level of sexual interest
ANXIETY SCALES Anxiety disorders are also highly prevalent in medial settings. Several assessment methods detect symptoms of anxiety. Generalized Anxiety Disorder Scale (GAD-7) Patient Health Questionnaire (PHQ-9)
REFERENCES Altmaier, E.M., & Tallman, B.A. (2013). Psychological assessment in medical settings. In APA Handbook of Testing and Assessment in Psychology: Volume 2. Testing and Assessment in Clinical and Counseling Psychology, 285-302). Bouchard, T.J. and McGue, M.J. (1981) Familial studies of intelligence: A review. Science, 1055-1059. Froehlich, L., Martiny, S.E., Keaux, K., Goetz, T., Mok, S.Y. (2016). Being smart of getting smarter. Implicit theory of intelligence moderates stereotype threat and stereotype lift effects. British Journal of Social Psychology, 55, 564-587. Haworth, C. M. A., Wright, M. J., Luciano, M., Martin, N. G., de Geus, E. J. C., van Beijsterveldt, C. E. M., . . . Plomin, R. (2010). The heritability of general cognitive ability increases linearly from childhood to young adulthood. Molecular Psychiatry, 15, 1112– 1120. Maltzman, S. (2013). The assessment process. In APA Handbook of Testing and Assessment in Psychology: Volume 2. Testing and Assessment in Clinical and Counseling Psychology, 19-34). Steele, C.M., & Aronson, J. (1995). Stereotype threat and the intellectual test performance of African Americans. Journal of Personality and Social Psychology, 69, 797-811.