Department of Hospital Epidemiology and Infection Control

27 Slides8.49 MB
Department of Hospital Epidemiology and Infection Control
Infection Control Contact Information Office Main Office: 350 Parnassus Ave, Suite 510 Mission Bay: 1855 Fourth St, Office 3626 Main Office Phone: 415-353-4343 Practitioner On-Call: 415-806-0269 Website Infection Control Manual includes all IC policies and other relevant Infection Control related information http://infectioncontrol.ucsfmedicalcenter.org
Hand Hygiene Institutional Goal 95% Observations of staff entering and exiting patient care areas
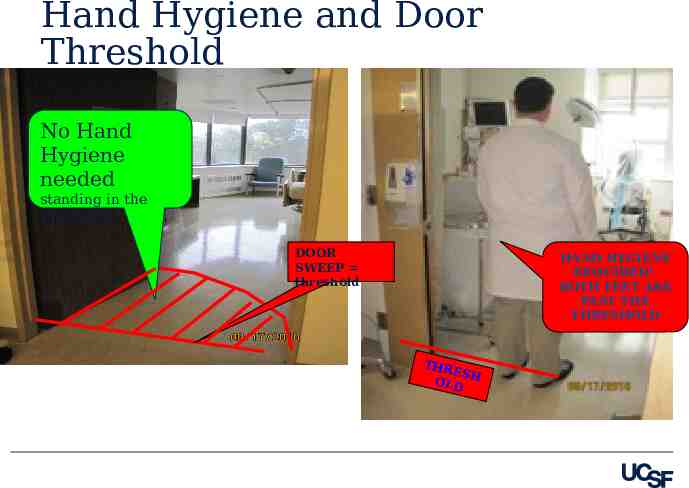
Hand Hygiene and Door Threshold No Hand Hygiene needed standing in the threshold DOOR SWEEP threshold HAND HYGIENE REQUIRED! BOTH FEET ARE PAST THE THRESHOLD THR ESH OLD
Which product should I use? Alcohol hand sanitizer For non visibly-soiled hands Use after removing gloves Use after dry skin contact Quick, effective, kind to skin More effective than soap and water for killing bacteria Infection Control
Which product should I use? USE SOAP AND WATER: Duration: 15 to 20 seconds When hands are visibly soiled Before preparing or eating food After using the restroom After caring for a patient with Clostridum difficile infection
Take a deep breath
Infection Control Program Identify patients with communicable diseases Prevent Hospital Acquired infections Ensure everyone understands infection control strategies Provide Education and Consultation
The Patients We Serve Acute care and tertiary referral center Immunocompromised patients Cancer Center Premature infants Majority of patients vulnerable to infections Referral center for complex patients from around the world
STANDARD PRECAUTIONS: Assess the patient and situation before providing care. Select and wear the best protection for yourself: Example: Dependent on Task – Splash risk emptying drainage bag. Wear gloves, gown and eye protection. Example: Dependent on patient condition – Coughing patient. Wear a mask with eye protection.
Standard Precautions Hand Hygiene, PPE, Surface Disinfection, Respiratory Etiquette . Used for every patient, every encounter Intended for the protection of the patients and the health care workers ‒ Patients are AT RISK for infection ‒ Patients can be THE SOURCE of infection
Personal Protective Equipment PPE Based on patient’s symptoms and diagnosis Better to be safe than sorry PPE is used to protect the health care provider and patients
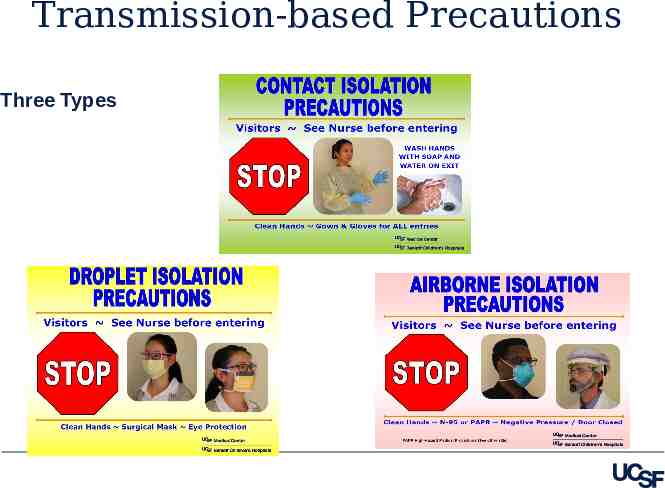
Transmission-based Precautions Three Types
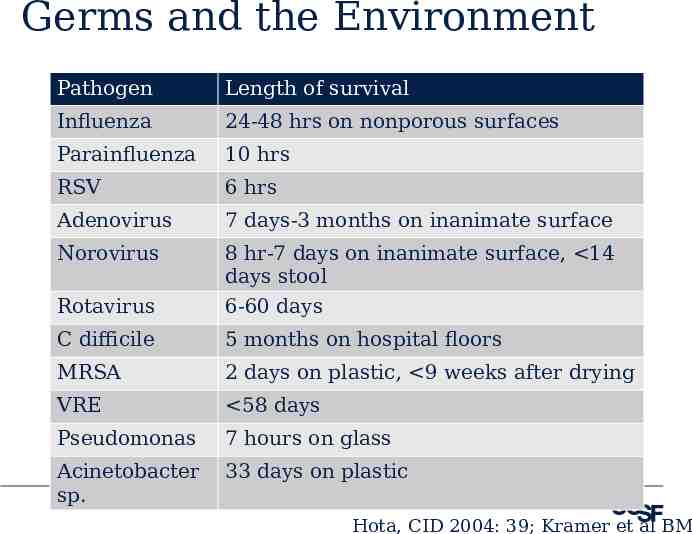
Germs and the Environment Pathogen Length of survival Influenza 24-48 hrs on nonporous surfaces Parainfluenza 10 hrs RSV 6 hrs Adenovirus 7 days-3 months on inanimate surface Norovirus 8 hr-7 days on inanimate surface, 14 days stool Rotavirus 6-60 days C difficile 5 months on hospital floors MRSA 2 days on plastic, 9 weeks after drying VRE 58 days Pseudomonas 7 hours on glass Acinetobacter sp. 33 days on plastic Hota, CID 2004: 39; Kramer et al BM
One of the most high touched surfaces
Surface Disinfection All patient care items and surfaces used for multiple patient contacts must be adequately surface disinfected between uses. Visible soiling must be removed. A hospital-approved detergent disinfectant must be applied and allowed to air dry before the next contact. Follow label directions for surface contact/air dry time Disinfect items you carry and/or use frequently regularly
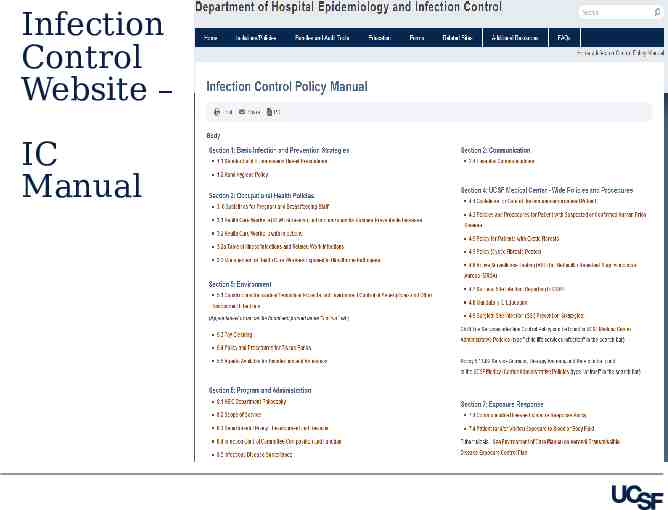
Infection Control Website http://infectioncontrol.ucsfmedicalcenter.org /
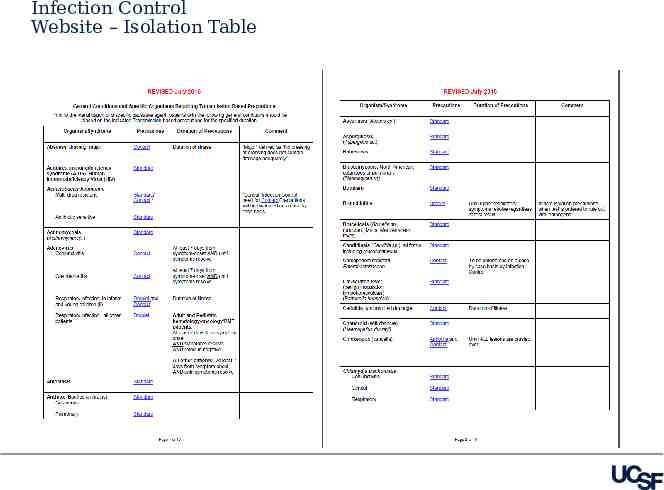
Infection Control Website – Isolation Table
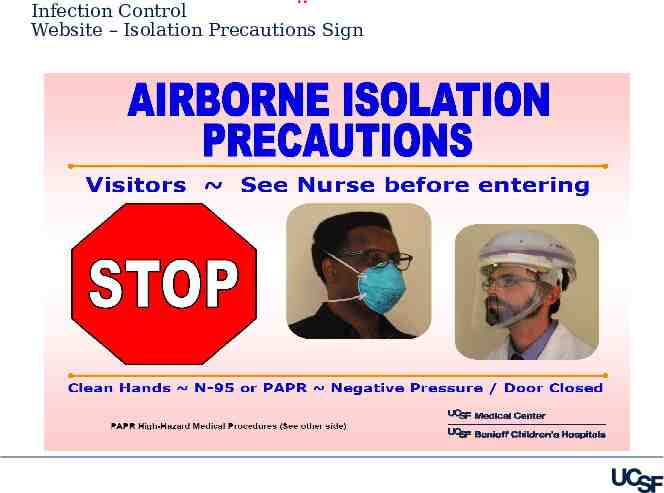
. Infection Control Website – Isolation Precautions Sign
Infection Control Website – IC Manual
Needle Stick Hot Line: Pager 353-STIC Following an exposure you should: Wash the area thoroughly with soap and water Report the injury to the Needle stick Hotline Inform your supervisor Report all needle sticks, lacerations and splashes 24-hour confidential assessment/triage, counseling, testing, treatment and information Prophylaxis and/or treatment available following work related exposures to blood-borne pathogens
Your Risk of Disease from an Exposure Approximate risk of transmission following exposure Hepatitis B – 6 – 30% depending on the source individual Hepatitis C –1.8% following needle stick or cut exposure HIV – 0.3% (needle stick), 0.09% (mucous membrane/splash)
Occupational Health Issues Illness and Work Restrictions: STAY HOME! Feel ill with fever, muscle aches, vomiting, diarrhea? Upper respiratory symptoms that may be contagious? Unexplained rash? Infection Control Policy Manual Section 3.2 Table of illness – Signs and symptoms when to stay home and when it is safe to return to work.
Healthy Tips: Self Care Always Work Well Diet Exercise Rest – Sleep FLU VACCINE
Tuberculosis – Patient on Airborne Precautions Transmits by breathing the germ Source must have active pulmonary disease to transmit Classic Symptoms Prolonged productive cough lasting 3 weeks Coughing up blood Weakness, weight loss, night sweats PPD Skin Test Annually (for patient care areas) PPD is a test for EXPOSURE (latent TB) 90% of PPD positive persons do NOT develop active TB
Respiratory Etiquette In waiting areas: Clinics, Doctor’s Office, Waiting Rooms Provide tissues and no touch receptacles for disposal Provide alcohol gel and make sure that appropriate supplies are always available in hand washing areas Offer masks to coughing patients; place immediately in exam rooms if possible Perform hand hygiene after contact with respiratory secretions and contaminated objects
The future of Infection Control technolog coming y your way soon!