Clinical Use and Benefit of HIV Surveillance Data Mary-Grace

32 Slides2.18 MB
Clinical Use and Benefit of HIV Surveillance Data Mary-Grace Brandt PhD MPH, Section Manager HIV/STD Surveillance and Epidemiology MDHHS
Outline The basics of HIV surveillance Outline how surveillance data supports HIV care and prevention goals New projects that use surveillance data Data to Care Molecular HIV Surveillance How these new projects support HIV care and prevention goals How HIV/STD care providers statewide can support new projects
Role of HIV Surveillance in Michigan The role of the MDHHS HIV/AIDS Surveillance Program is to monitor the HIV/AIDS epidemic in Michigan, analyze trends in HIV diagnoses and disease morbidity, and provide accurate and complete data for prevention initiatives and care activities.
HIV Case Finding in Michigan All laboratories and rapid-testing sites nationwide that run detection tests on Michigan residents have been required to report HIV-related results since April 2005 (MCL 333.5114) Alere Determine, Insti WBs, 4th generation lab detection tests Type Differentiating tests: Geenius Viral Loads CD4 counts and percents Genotypes Electronic Matches NDI, SSDI, Cancer, STD, Prison, TB, Viral Hep Provider-Surveillance Relationships Staff can request site line and discharge lists for case finding Staff are assigned to sites by county and health system
Case Reporting Laboratory Management System (LMS) Manages all electronic lab reports Each surveillance staff member has a queue Allow us to share lab reports with LHDs Paper CRFs Provides check/balance with labs from LMS Used when testing is done via dual-rapids MDSS Provides check/balance with labs from LMS Used for all other communicable diseases including STDs
Successes – Quality Data! Case reporting completeness: 95% for last 10 years 98.7% for 2017 Timeliness: over 95% for last 10 years 98.6% for 2017 Duplicates: 0.1% for last 10 years 0 duplicates in 2017 As of July 2017, 82.9% of persons diagnosed in the past 12 months had a reported CD4 or Viral Load Result within 3 months of diagnosis In 2017, 98.9% of new surveillance records pass standard CDC data quality checks
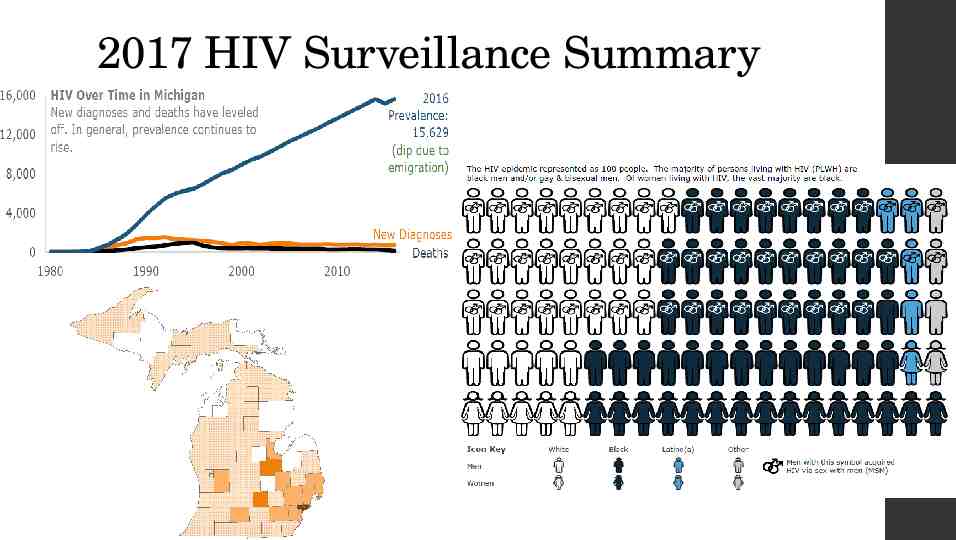
2017 HIV Surveillance Summary
Data reports and projects www.Michigan.gov/hivstd HIV Case Reporting and Data HIV Statistics and Data Reports
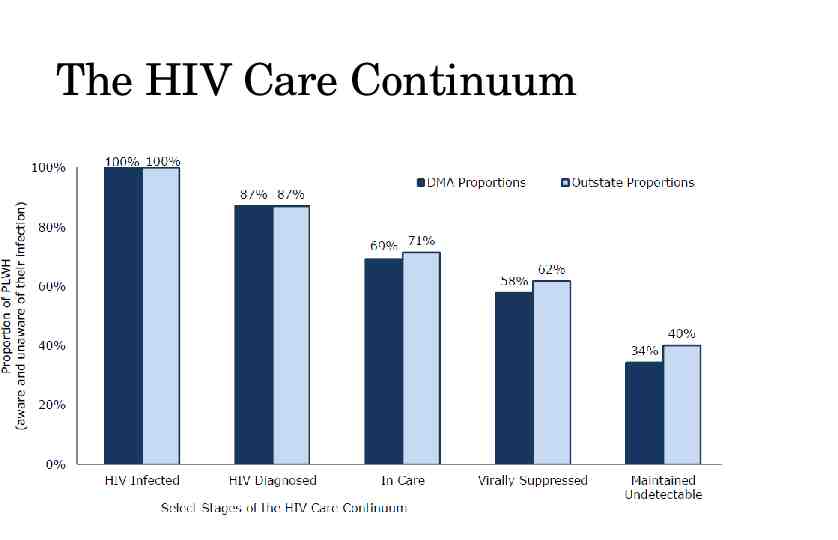
The HIV Care Continuum
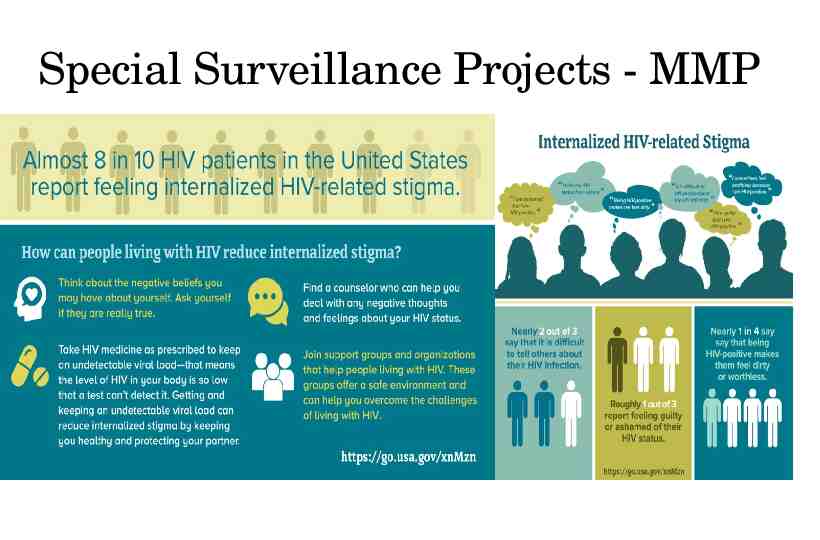
Special Surveillance Projects - MMP
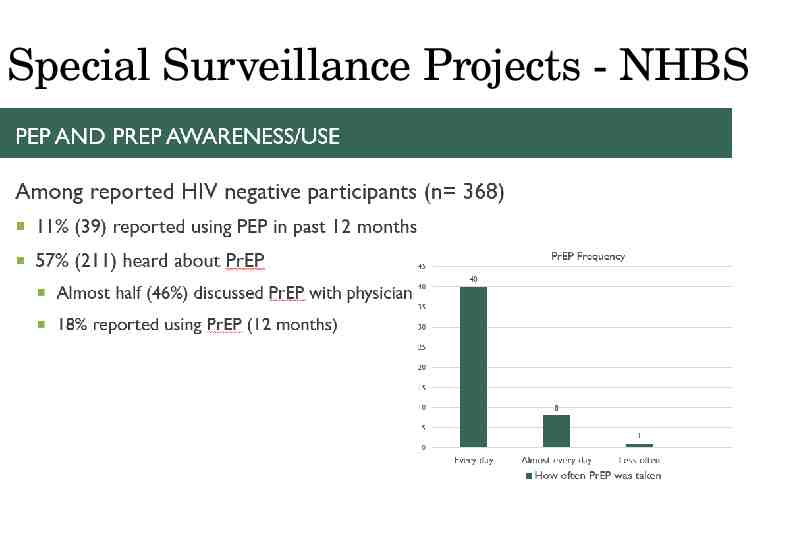
Special Surveillance Projects - NHBS
Data to Care
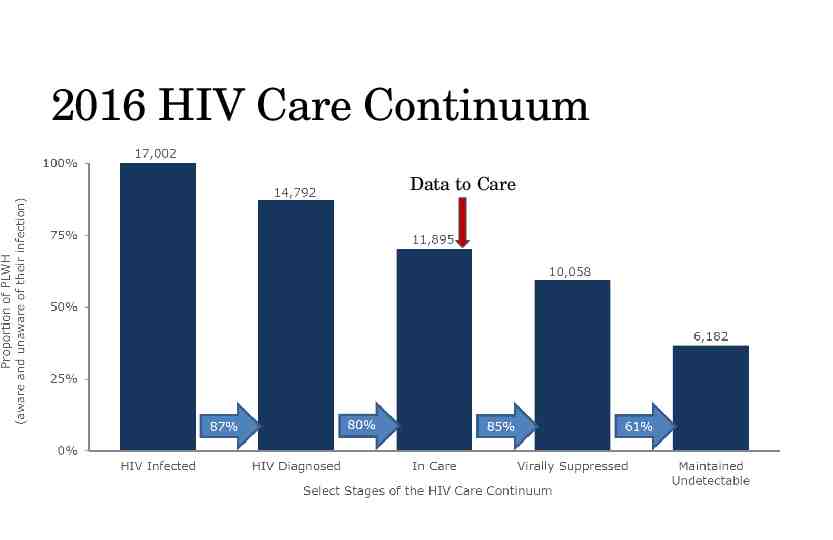
Data 2 Care in Michigan (LINK UP MI) CDC definition: “Data to Care is a new public health strategy that aims to use HIV surveillance data to identify HIV-diagnosed individuals not in care, link them to care, and support the HIV Care Continuum.” Basic Concept: In Michigan, HIV labs are reported to MDHHS Lab reports are used as a proxy to determine if an HIV-positive individual has been to a medical appointment for their HIV infection If some appears to be out of care MDHHS sends contact information (name, phone # address, place/date of diagnosis) to the local health department The local health department reaches out to these individuals to offer reengagement into HIV medical care and support services The local health department reports re-engagements efforts back to MDHHS 13
2016 HIV Care Continuum Data to Care
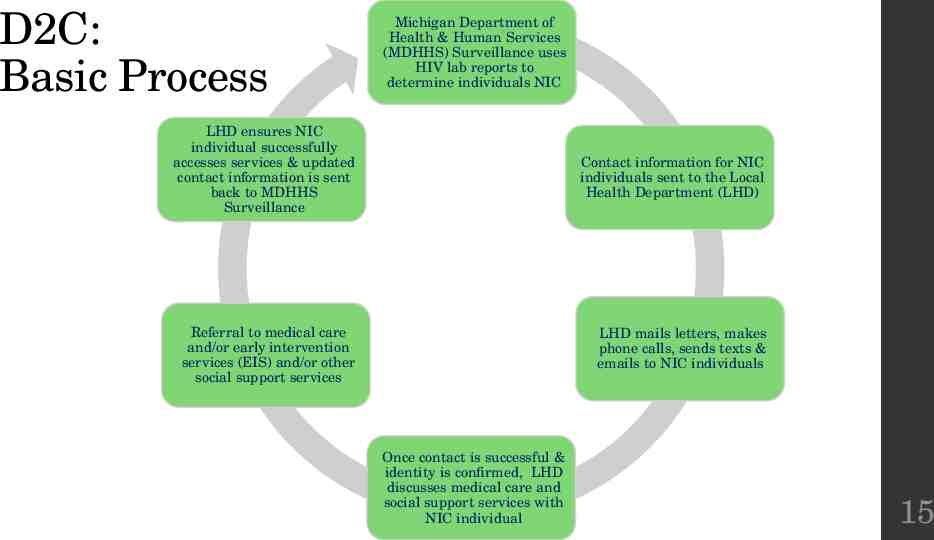
D2C: Basic Process Michigan Department of Health & Human Services (MDHHS) Surveillance uses HIV lab reports to determine individuals NIC LHD ensures NIC individual successfully accesses services & updated contact information is sent back to MDHHS Surveillance Contact information for NIC individuals sent to the Local Health Department (LHD) Referral to medical care and/or early intervention services (EIS) and/or other social support services LHD mails letters, makes phone calls, sends texts & emails to NIC individuals Once contact is successful & identity is confirmed, LHD discusses medical care and social support services with NIC individual 15
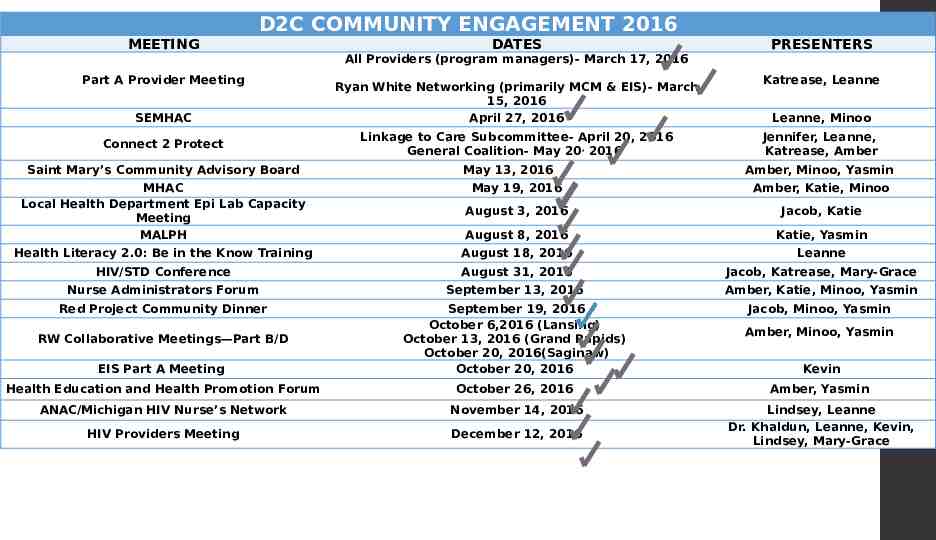
D2C COMMUNITY ENGAGEMENT 2016 MEETING DATES PRESENTERS All Providers (program managers)- March 17, 2016 Part A Provider Meeting SEMHAC Connect 2 Protect Saint Mary’s Community Advisory Board Ryan White Networking (primarily MCM & EIS)- March 15, 2016 April 27, 2016 Linkage to Care Subcommittee- April 20, 2016 General Coalition- May 20, 2016 May 13, 2016 Katrease, Leanne Leanne, Minoo Jennifer, Leanne, Katrease, Amber Amber, Minoo, Yasmin MHAC Local Health Department Epi Lab Capacity Meeting MALPH May 19, 2016 Amber, Katie, Minoo August 3, 2016 Jacob, Katie August 8, 2016 Katie, Yasmin Health Literacy 2.0: Be in the Know Training August 18, 2016 Leanne HIV/STD Conference August 31, 2016 Jacob, Katrease, Mary-Grace Nurse Administrators Forum September 13, 2016 Amber, Katie, Minoo, Yasmin Red Project Community Dinner Jacob, Minoo, Yasmin EIS Part A Meeting September 19, 2016 October 6,2016 (Lansing) October 13, 2016 (Grand Rapids) October 20, 2016(Saginaw) October 20, 2016 Health Education and Health Promotion Forum October 26, 2016 Amber, Yasmin ANAC/Michigan HIV Nurse’s Network November 14, 2016 HIV Providers Meeting December 12, 2016 Lindsey, Leanne Dr. Khaldun, Leanne, Kevin, Lindsey, Mary-Grace RW Collaborative Meetings—Part B/D Amber, Minoo, Yasmin Kevin
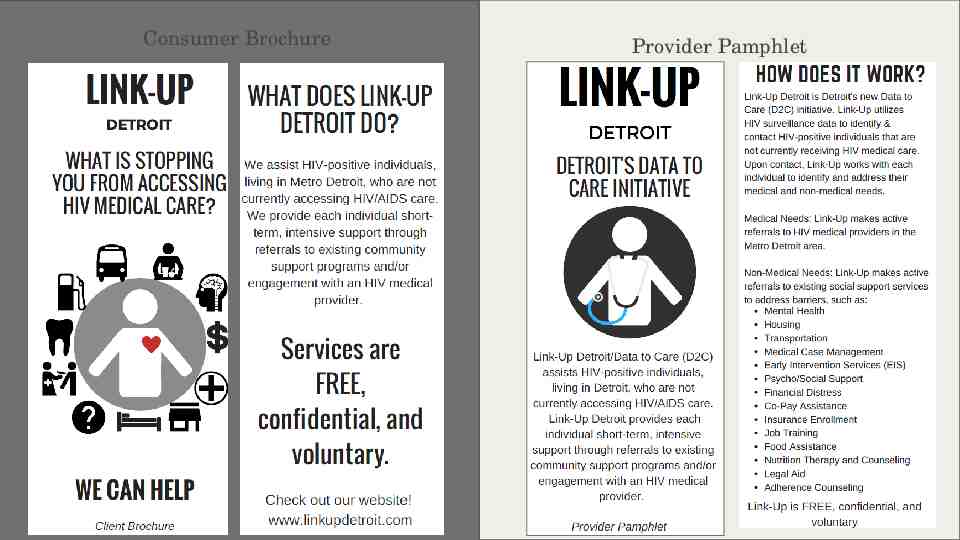
Consumer Brochure Provider Pamphlet
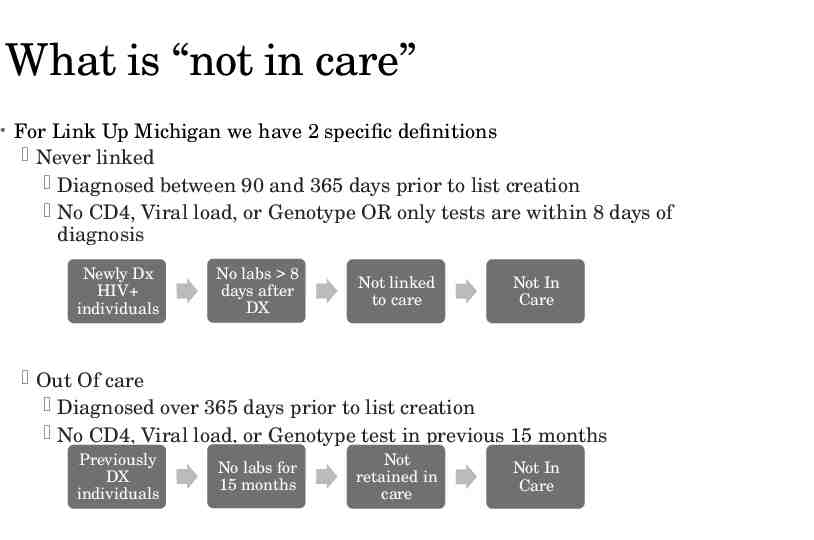
What is “not in care” For Link Up Michigan we have 2 specific definitions Never linked Diagnosed between 90 and 365 days prior to list creation No CD4, Viral load, or Genotype OR only tests are within 8 days of diagnosis Newly Dx HIV individuals No labs 8 days after DX Not linked to care Not In Care Out Of care Diagnosed over 365 days prior to list creation No CD4, Viral load, or Genotype test in previous 15 months Previously DX individuals No labs for 15 months Not retained in care Not In Care
What is Shared with LHDs? As mentioned earlier HIV individuals never linked HIV individuals that have fallen out of care Variables that help the D2C/Link Up Michigan process Phone numbers, addresses, and diagnosing facility Variables that MDHHS needs updated Race, sex, risk, address, phone numbers When the lists are sent any individual that has a missing field for risk or race should be priority to update
What are the Priorities? Surveillance uses SAS code to create the lists Most recent lab(CD4, Geno, VL) is pulled to determine NIC status NIC list is matched to STD data Lists are then prioritized by: Those newly DX Linkage status STD in the past 6 months Age ( 25) Transgender status VL within past 3 years VL greater than past 3 years
Data Returns to Surveillance An updated case report form is completed when an out of care individual is successfully engaged by the D2C team Updated demographics Risk Testing and Treatment History (including use of ARV) Current or last site of care and labs A database is maintained that examines barriers to care and successful engagement strategies, provides a comprehensive needs assessment, and suggests factors that may be associated with successful achievement of viral suppression
How Can YOU Support Link Up Michigan? Be Informed! Talk it UP! We get referrals Refer to our website www.linkupdetroit.com
Molecular HIV Surveillance
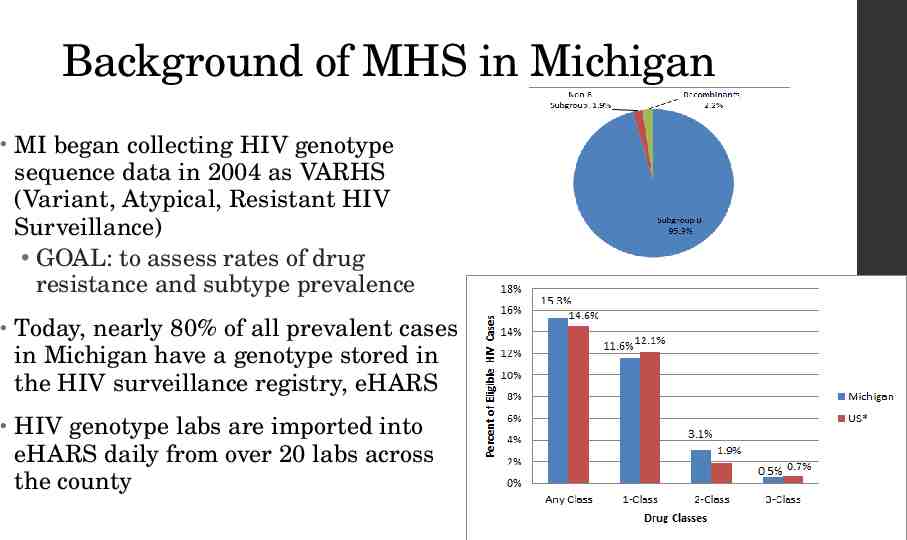
Background of MHS in Michigan MI began collecting HIV genotype sequence data in 2004 as VARHS (Variant, Atypical, Resistant HIV Surveillance) GOAL: to assess rates of drug resistance and subtype prevalence Today, nearly 80% of all prevalent cases in Michigan have a genotype stored in the HIV surveillance registry, eHARS HIV genotype labs are imported into eHARS daily from over 20 labs across the county
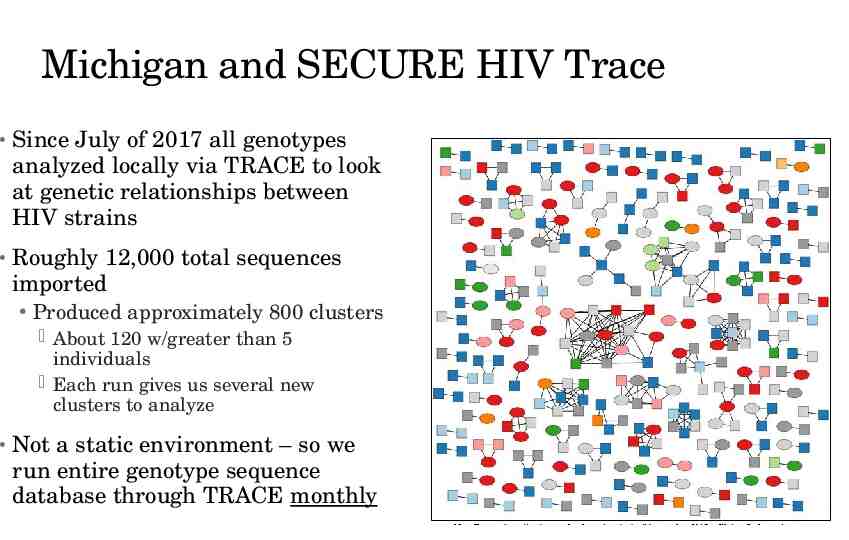
Michigan and SECURE HIV Trace Since July of 2017 all genotypes analyzed locally via TRACE to look at genetic relationships between HIV strains Roughly 12,000 total sequences imported Produced approximately 800 clusters About 120 w/greater than 5 individuals Each run gives us several new clusters to analyze Not a static environment – so we run entire genotype sequence database through TRACE monthly
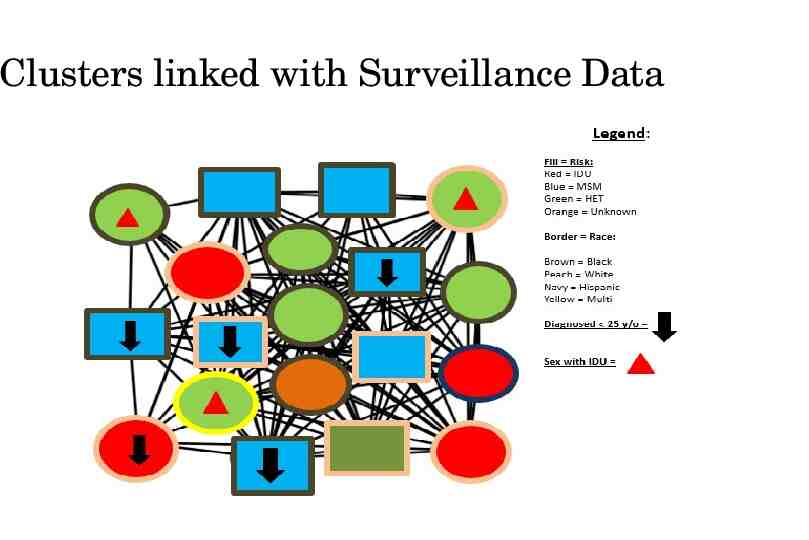
Clusters linked with Surveillance Data
Clusters are Prioritized Must have at least 3 new cases in past year All cases with date of dx in past 3 years included in cluster intervention Clusters with new cases are prioritized by: High VL Status of Not in care (NIC) STD Co-infection No evidence of Partner Service or DIS counseling Partner Services database and MDSS (local disease surveillance system) used to add supplemental info: If they were interviewed by PS How many partners identified
The Roll Out to LHDs Big picture is shared with HIV prevention staff to understand general trends in new diagnoses Line lists are shared with local health department to discuss possible interventions The Foundation: Multiple presentations and community engagement events Developed a technical guidance document that is posted on our website – www.Michigan.gov/hivstd Distributed letters to all LHDs, CBOs and Providers outlining MHS goals Developed Protocol and Scrips with the help of community advocates
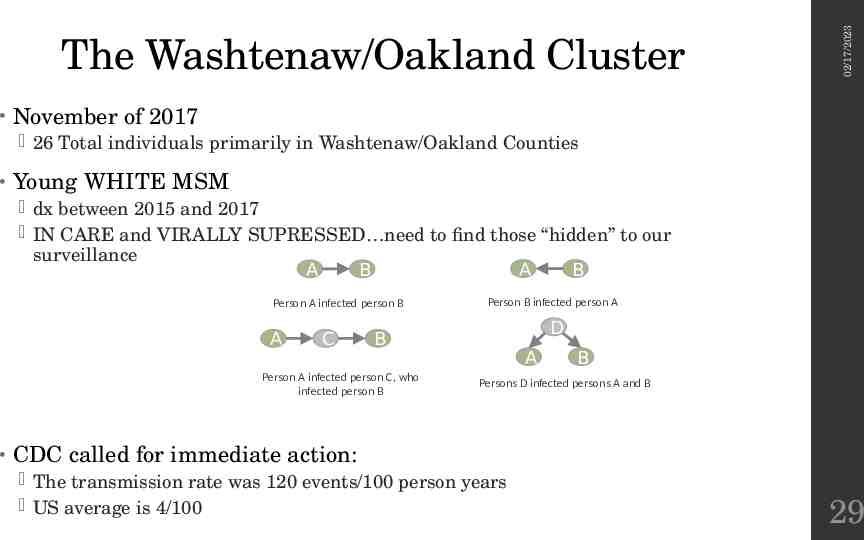
02/17/2023 The Washtenaw/Oakland Cluster November of 2017 26 Total individuals primarily in Washtenaw/Oakland Counties Young WHITE MSM dx between 2015 and 2017 IN CARE and VIRALLY SUPRESSED need to find those “hidden” to our surveillance A B A B Person A infected person B A C D B Person A infected person C, who infected person B Person B infected person A A B Persons D infected persons A and B CDC called for immediate action: The transmission rate was 120 events/100 person years US average is 4/100 29
Met with LHDs – developed plan centered around providers (in care!) The index clients/partners who did not receive an interview by were given priority and calls were placed directly to these individuals For index clients who already were interviewed Call was placed to their ID provider to discuss MHS A copy of the MDHHS letter and an LHD molecular cluster letter, addressed to the client, was faxed to the provider The providers agreed to have a conversation with their patient at their next visit regarding the molecular cluster and the importance of PS Providers asked to encourage patients to contact LHD for PS 02/17/2023 The Washtenaw/Oakland Cluster 30
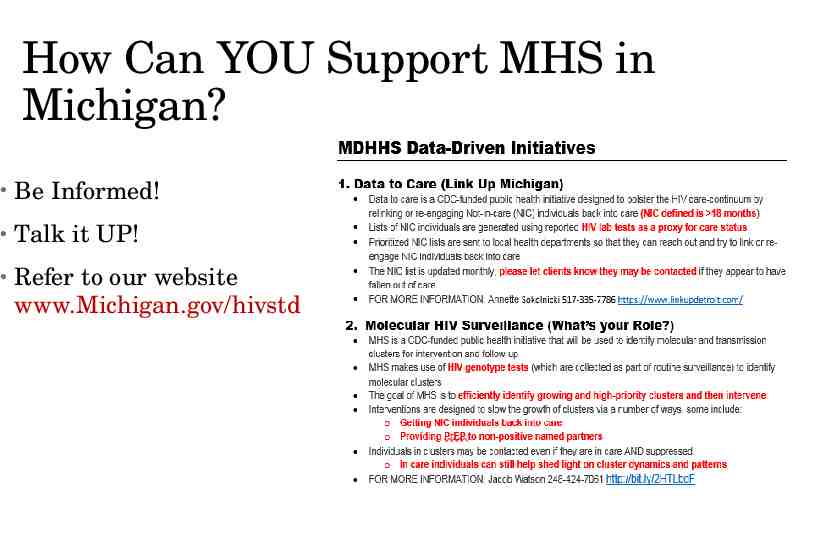
How Can YOU Support MHS in Michigan? Be Informed! Talk it UP! Refer to our website www.Michigan.gov/hivstd
Thank You! CONTACT INFORMATION: Mary-Grace Brandt 248 424-7913 [email protected]