CheckMate 227 CT077 2018 CHICAGO, IL Nivolumab + Ipilimumab


56 Slides3.27 MB
CheckMate 227 CT077 2018 CHICAGO, IL Nivolumab Ipilimumab vs Platinum-Doublet Chemotherapy as First-line Treatment for Advanced Non-Small Cell Lung Cancer: Initial Results From CheckMate 227 Matthew D. Hellmann,1 Tudor-Eliade Ciuleanu,2 Adam Pluzanski,3 Jong Seok Lee,4 Gregory A. Otterson,5 Clarisse Audigier-Valette,6 Elisa Minenza,7 Helena Linardou,8 Sjaak Burgers,9 Pamela Salman,10 Hossein Borghaei,11 Suresh S. Ramalingam,12 Julie Brahmer,13 Martin Reck,14 Kenneth J. O’Byrne,15 William J. Geese,16 George Green,16 Han Chang,16 Joseph Szustakowski,16 Prabhu Bhagavatheeswaran,16 Diane Healey,16 Yali Fu,16 Faith Nathan,16 Luis Paz-Ares17 1 Memorial Sloan Kettering Cancer Center Hospital, New York, NY, USA; 2Prof. Dr. Ion Chiricuta Institute of Oncology and Universitatea de Medicina si Farmacie Iuliu Hatieganu, Cluj-napoca, Romania; 3Centrum Onkologii–Instytut im. Marii Sklodowskiej-Curie, Warsaw, Poland; 4Seoul National University Bundang Hospital, Seoul, South Korea; 5The Ohio State University, Columbus, OH, USA; 6Hôpital Sainte Musse, Toulon, France; 7Ospedale Santa Maria della Misericordia, Perugia, Italy; 8First Department of Oncology, Metropolitan Hospital, Athens, Greece; 9Antoni Van Leeuwenhoek Ziekenhuis, Amsterdam, the Netherlands; 10Fundación Arturo López Pérez, Santiago, Chile; 11Fox Chase Cancer Center, Philadelphia, PA, USA; 12Winship Cancer Institute, Emory University, Atlanta, GA, USA; 13Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA; 14LungenClinic Grosshansdorf, Airway Research Center North, German Center for Lung Research, Grosshansdorf, Germany; 15Princess Alexandra Hospital, Brisbane, QLD, Australia; 16Bristol-Myers Squibb, Princeton, NJ, USA; 17Hospital Universitario 12 de Octubre, Centro Nacional de Investigaciones Oncológicas, Universidad Complutense, & CiberOnc, Madrid, Spain
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Disclosure Information Matthew D. Hellmann, MD I have the following financial relationships to disclose: Consultant for: AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, Janssen, Merck, Mirati Therapeutics, Novartis, and Shattuck Labs Grant/Research support from: Bristol-Myers Squibb I will discuss the following off label use and/or investigational use in my presentation: First-line treatment of NSCLC with nivolumab ipilimumab 2
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Introduction The standard-of-care first-line treatment for patients with advanced NSCLC has been characterized by platinum-doublet chemotherapy or pembrolizumab in patients with 50% tumor PD-L1 expression 1-3 Nivolumab and ipilimumab are immune checkpoint inhibitor antibodies with distinct but complementary mechanisms of action Nivolumab ipilimumab demonstrated improved survival in phase 3 studies in melanoma and RCC 4,5 CheckMate 012 evaluated nivolumab ipilimumab in first-line NSCLC 6,7 – Dosing of nivolumab 3 mg/kg Q2W ipilimumab 1 mg/kg Q6W was optimized for NSCLC (13% discontinuation due to TRAEs in nivolumab low-dose ipilimumab) – Nivolumab ipilimumab demonstrated improved outcomes relative to nivolumab – Efficacy was enhanced in patients with 1% tumor PD-L1 expression 1. Ettinger DS, et al. J Natl Compr Canc Netw 2016;14:255–264; 2. Masters GA, et al. J Clin Oncol 2015;33:3488–3515; 3. Reck M, et al. N Engl J Med 2016;375:1823–1833; 4. Wolchock JD, et al. N Engl J Med 2017;377:1345–1356; 5. Escudier B, et al. Ann Oncol 2017;28(Suppl 5): Abstract LBA5; 6. Hellmann MD, et al. Lancet Oncol 2017;18:31–41; 7. Goldman JW, et al. Poster presentation at ASCO 2017 Annual Meeting; June 2–6, 2017; Chicago, IL, USA. Abstract 9093. 3
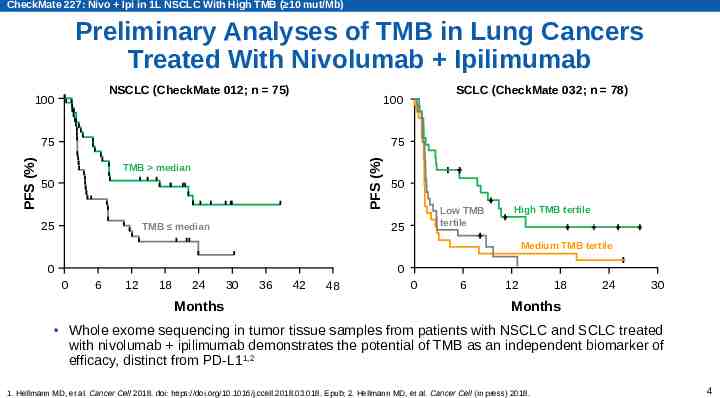
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Preliminary Analyses of TMB in Lung Cancers Treated With Nivolumab Ipilimumab NSCLC (CheckMate 012; n 75) 100 75 75 PFS (%) PFS (%) SCLC (CheckMate 032; n 78) 100 TMB median 50 25 50 Low TMB tertile 25 TMB median High TMB tertile Medium TMB tertile 0 0 0 6 12 18 24 Months 30 36 42 48 0 6 12 18 24 30 Months Whole exome sequencing in tumor tissue samples from patients with NSCLC and SCLC treated with nivolumab ipilimumab demonstrates the potential of TMB as an independent biomarker of efficacy, distinct from PD-L11,2 1. Hellmann MD, et al. Cancer Cell 2018. doi: https://doi.org/10.1016/j.ccell.2018.03.018. Epub; 2. Hellmann MD, et al. Cancer Cell (in press) 2018. 4
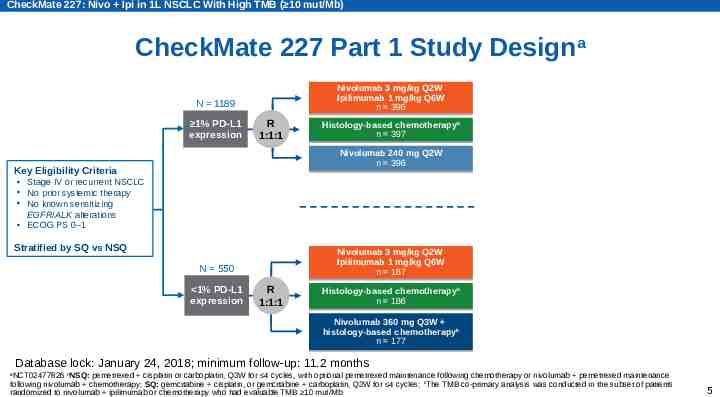
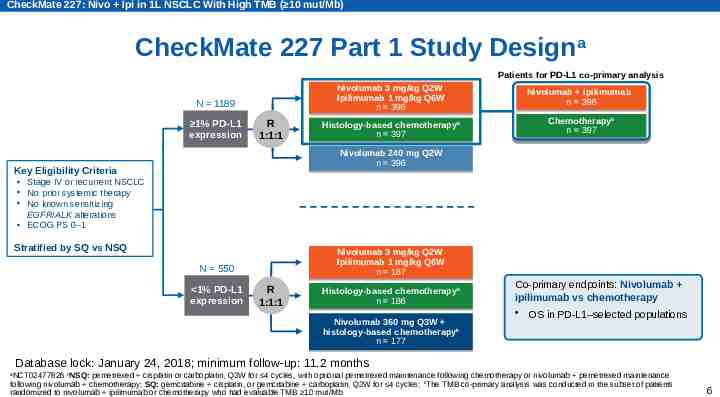
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227 Part 1 Study Designa Nivolumab Nivolumab 3 3 mg/kg mg/kg Q2W Q2W Ipilimumab 1 mg/kg Q6W n 396 N 1189 1% PD-L1 expression R 1:1:1 Histology-based chemotherapybb n 397 Nivolumab 240 mg Q2W n 396 Key Eligibility Criteria Stage IV or recurrent NSCLC No prior systemic therapy No known sensitizing EGFR/ALK alterations ECOG PS 0–1 Stratified by SQ vs NSQ Nivolumab 3 mg/kg Q2W Ipilimumab 1 mg/kg Q6W n 187 N 550 1% PD-L1 expression R 1:1:1 Histology-based chemotherapybb n 186 Nivolumab Nivolumab 360 360 mg mg Q3W Q3W b histology-based histology-based chemotherapy chemotherapyb n n 177 177 Database lock: January 24, 2018; minimum follow-up: 11.2 months NCT02477826 bNSQ: pemetrexed cisplatin or carboplatin, Q3W for 4 cycles, with optional pemetrexed maintenance following chemotherapy or nivolumab pemetrexed maintenance following nivolumab chemotherapy; SQ: gemcitabine cisplatin, or gemcitabine carboplatin, Q3W for 4 cycles; cThe TMB co-primary analysis was conducted in the subset of patients randomized to nivolumab ipilimumab or chemotherapy who had evaluable TMB 10 mut/Mb a 5
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227 Part 1 Study Designa Patients for PD-L1 co-primary analysis N 1189 1% PD-L1 expression R 1:1:1 Nivolumab Nivolumab 3 3 mg/kg mg/kg Q2W Q2W Ipilimumab 1 mg/kg Q6W n 396 Nivolumab Nivolumab ipilimumab ipilimumab n n 396 396 Histology-based chemotherapybb n 397 Chemotherapybb n n 397 397 Nivolumab 240 mg Q2W n 396 Key Eligibility Criteria Stage IV or recurrent NSCLC No prior systemic therapy No known sensitizing EGFR/ALK alterations ECOG PS 0–1 Stratified by SQ vs NSQ Nivolumab 3 mg/kg Q2W Ipilimumab 1 mg/kg Q6W n 187 N 550 1% PD-L1 expression R 1:1:1 Histology-based chemotherapybb n 186 Nivolumab Nivolumab 360 360 mg mg Q3W Q3W b histology-based histology-based chemotherapy chemotherapyb n n 177 177 Co-primary endpoints: Nivolumab ipilimumab vs chemotherapy OS in PD-L1–selected populations Database lock: January 24, 2018; minimum follow-up: 11.2 months NCT02477826 bNSQ: pemetrexed cisplatin or carboplatin, Q3W for 4 cycles, with optional pemetrexed maintenance following chemotherapy or nivolumab pemetrexed maintenance following nivolumab chemotherapy; SQ: gemcitabine cisplatin, or gemcitabine carboplatin, Q3W for 4 cycles; cThe TMB co-primary analysis was conducted in the subset of patients randomized to nivolumab ipilimumab or chemotherapy who had evaluable TMB 10 mut/Mb a 6
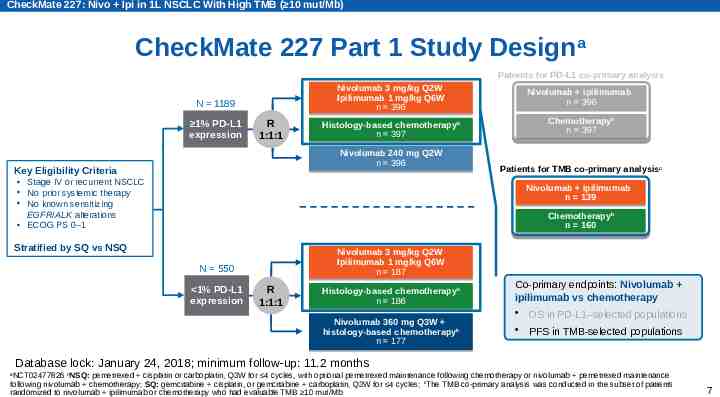
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227 Part 1 Study Designa Patients for PD-L1 co-primary analysis N 1189 1% PD-L1 expression R 1:1:1 Nivolumab Nivolumab 3 3 mg/kg mg/kg Q2W Q2W Ipilimumab 1 mg/kg Q6W n 396 Nivolumab Nivolumab ipilimumab ipilimumab n n 396 396 Histology-based chemotherapybb n 397 Chemotherapybb n n 397 397 Nivolumab 240 mg Q2W n 396 Key Eligibility Criteria Stage IV or recurrent NSCLC No prior systemic therapy No known sensitizing EGFR/ALK alterations ECOG PS 0–1 Patients for TMB co-primary analysisc Nivolumab ipilimumab n 139 Chemotherapy Chemotherapybb n 160 Stratified by SQ vs NSQ Nivolumab 3 mg/kg Q2W Ipilimumab 1 mg/kg Q6W n 187 N 550 1% PD-L1 expression R 1:1:1 Histology-based chemotherapybb n 186 Nivolumab Nivolumab 360 360 mg mg Q3W Q3W b histology-based histology-based chemotherapy chemotherapyb n n 177 177 Co-primary endpoints: Nivolumab ipilimumab vs chemotherapy OS in PD-L1–selected populations PFS in TMB-selected populations Database lock: January 24, 2018; minimum follow-up: 11.2 months NCT02477826 bNSQ: pemetrexed cisplatin or carboplatin, Q3W for 4 cycles, with optional pemetrexed maintenance following chemotherapy or nivolumab pemetrexed maintenance following nivolumab chemotherapy; SQ: gemcitabine cisplatin, or gemcitabine carboplatin, Q3W for 4 cycles; cThe TMB co-primary analysis was conducted in the subset of patients randomized to nivolumab ipilimumab or chemotherapy who had evaluable TMB 10 mut/Mb a 7
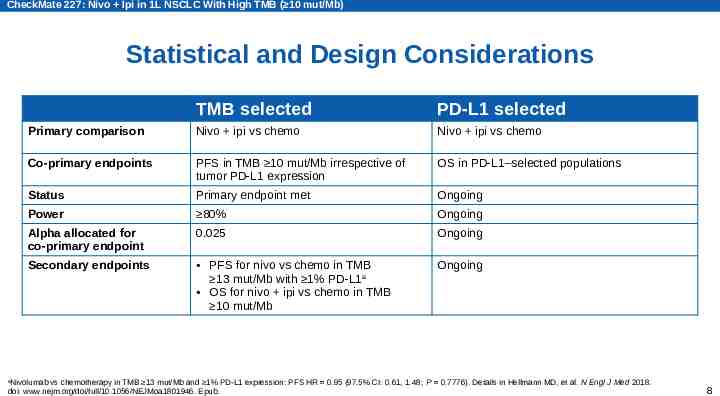
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Statistical and Design Considerations TMB selected PD-L1 selected Primary comparison Nivo ipi vs chemo Nivo ipi vs chemo Co-primary endpoints PFS in TMB 10 mut/Mb irrespective of tumor PD-L1 expression OS in PD-L1–selected populations Status Primary endpoint met Ongoing Power 80% Ongoing Alpha allocated for co-primary endpoint 0.025 Ongoing Secondary endpoints PFS for nivo vs chemo in TMB 13 mut/Mb with 1% PD-L1 a OS for nivo ipi vs chemo in TMB 10 mut/Mb Ongoing Nivolumab vs chemotherapy in TMB 13 mut/Mb and 1% PD-L1 expression: PFS HR 0.95 (97.5% CI: 0.61, 1.48; P 0.7776). Details in Hellmann MD, et al. N Engl J Med 2018. doi: www.nejm.org/doi/full/10.1056/NEJMoa1801946. Epub. a 8
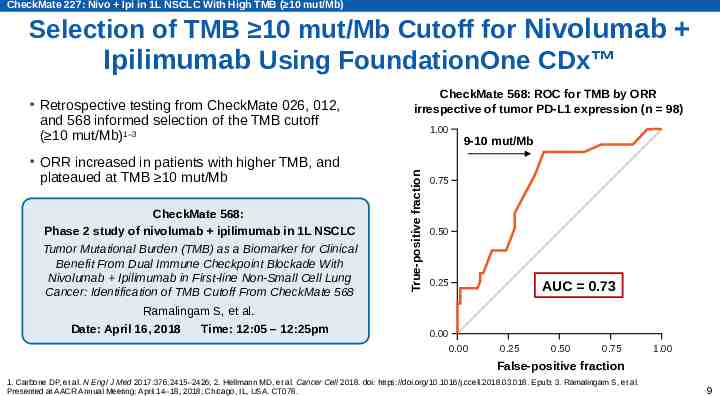
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Selection of TMB 10 mut/Mb Cutoff for Nivolumab Ipilimumab Using FoundationOne CDx ORR increased in patients with higher TMB, and plateaued at TMB 10 mut/Mb CheckMate 568: Phase 2 study of nivolumab ipilimumab in 1L NSCLC Tumor Mutational Burden (TMB) as a Biomarker for Clinical Benefit From Dual Immune Checkpoint Blockade With Nivolumab Ipilimumab in First-line Non-Small Cell Lung Cancer: Identification of TMB Cutoff From CheckMate 568 CheckMate 568: ROC for TMB by ORR irrespective of tumor PD-L1 expression (n 98) 1.00 True-positive fraction Retrospective testing from CheckMate 026, 012, and 568 informed selection of the TMB cutoff ( 10 mut/Mb)1–3 9-10 mut/Mb 0.75 0.50 0.25 AUC 0.73 Ramalingam S, et al. Date: April 16, 2018 Time: 12:05 – 12:25pm 0.00 0.00 0.25 0.50 0.75 1.00 False-positive fraction 1. Carbone DP, et al. N Engl J Med 2017:376;2415–2426; 2. Hellmann MD, et al. Cancer Cell 2018. doi: https://doi.org/10.1016/j.ccell.2018.03.018. Epub; 3. Ramalingam S, et al. Presented at AACR Annual Meeting; April 14–18, 2018; Chicago, IL, USA. CT078. 9
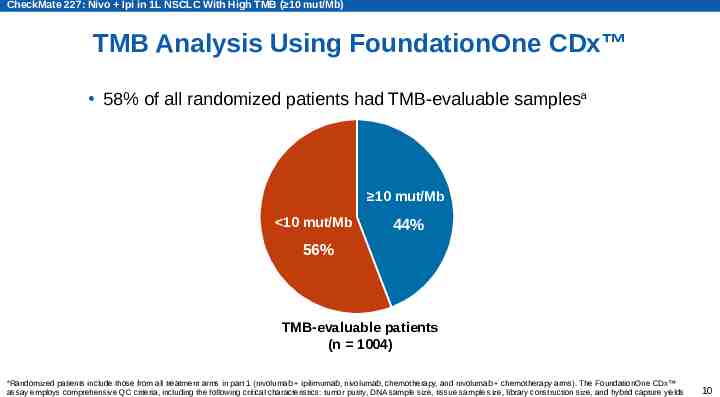
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) TMB Analysis Using FoundationOne CDx 58% of all randomized patients had TMB-evaluable samplesa 10 mut/Mb 10 mut/Mb 44% 56% TMB-evaluable patients (n 1004) Randomized patients include those from all treatment arms in part 1 (nivolumab ipilimumab, nivolumab, chemotherapy, and nivolumab chemotherapy arms). The FoundationOne CDx assay employs comprehensive QC criteria, including the following critical characteristics: tumor purity, DNA sample size, tissue sample size, library construction size, and hybrid capture yields a 10
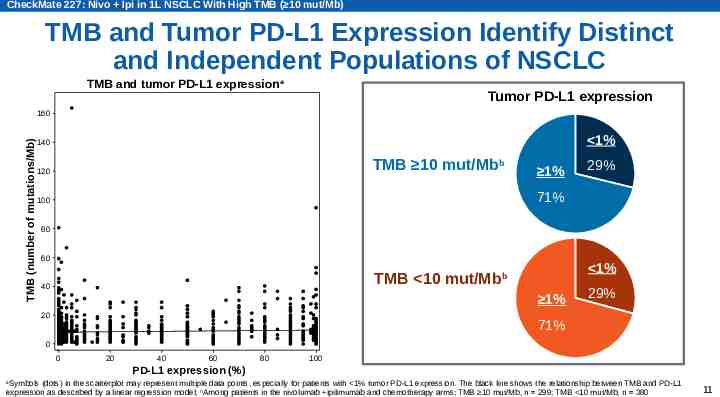
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) TMB and Tumor PD-L1 Expression Identify Distinct and Independent Populations of NSCLC TMB and tumor PD-L1 expression a Tumor PD-L1 expression TMB (number of mutations/Mb) 160 140 TMB 10 mut/Mbb 120 1% 1% 29% 29% 1% 1% 71% 71% 100 80 60 1% 1% TMB 10 mut/Mbb 40 1% 1% 71% 71% 20 29% 29% 0 0 20 40 60 80 100 PD-L1 expression (%) Symbols (dots) in the scatterplot may represent multiple data points, especially for patients with 1% tumor PD-L1 expression. The black line shows the relationship between TMB and PD-L1 expression as described by a linear regression model; bAmong patients in the nivolumab ipilimumab and chemotherapy arms; TMB 10 mut/Mb, n 299; TMB 10 mut/Mb, n 380 a 11
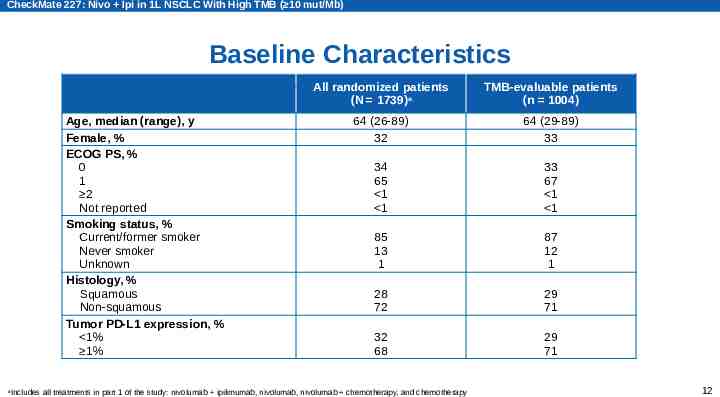
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Baseline Characteristics Age, median (range), y Female, % ECOG PS, % 0 1 2 Not reported Smoking status, % Current/former smoker Never smoker Unknown Histology, % Squamous Non-squamous Tumor PD-L1 expression, % 1% 1% a All randomized patients (N 1739)a TMB-evaluable patients (n 1004) 64 (26-89) 32 64 (29-89) 33 34 65 1 1 33 67 1 1 85 13 1 87 12 1 28 72 29 71 32 68 29 71 Includes all treatments in part 1 of the study: nivolumab ipilimumab, nivolumab, nivolumab chemotherapy, and chemotherapy 12
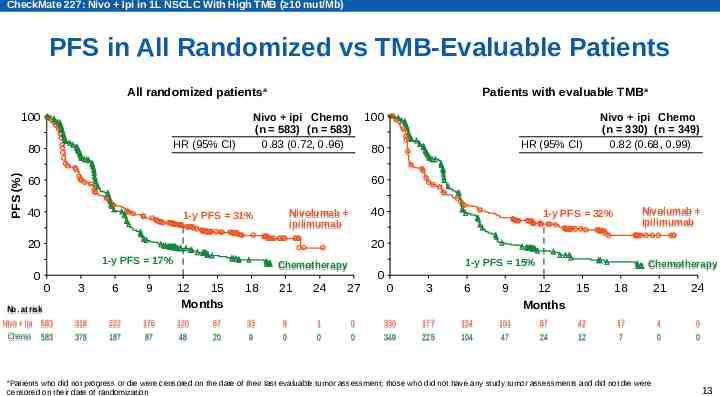
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) PFS in All Randomized vs TMB-Evaluable Patients All randomized patientsa 100 HR (95% CI) PFS (%) 80 Patients with evaluable TMB a Nivo ipi Chemo (n 583) (n 583) 0.83 (0.72, 0.96) HR (95% CI) 80 Nivo ipi Chemo (n 330) (n 349) 0.82 (0.68, 0.99) 60 60 40 40 Nivolumab ipilimumab 1-y PFS 31% Nivolumab ipilimumab 1-y PFS 32% 20 20 1-y PFS 17% 0 100 0 No. at risk Nivo Nivo ipi ipi 583 583 Chemo 583 583 3 6 9 318 318 376 376 222 222 187 187 176 176 87 87 1-y PFS 15% Chemotherapy 12 15 Months 18 21 24 27 120 120 48 48 33 33 99 99 00 11 00 00 00 67 67 20 20 0 0 3 6 9 330 330 349 349 177 177 225 225 124 124 104 104 101 101 47 47 Chemotherapy 12 15 Months 67 67 24 24 42 42 12 12 18 21 24 17 17 77 44 00 00 00 Patients who did not progress or die were censored on the date of their last evaluable tumor assessment; those who did not have any study tumor assessments and did not die were censored on their date of randomization a 13
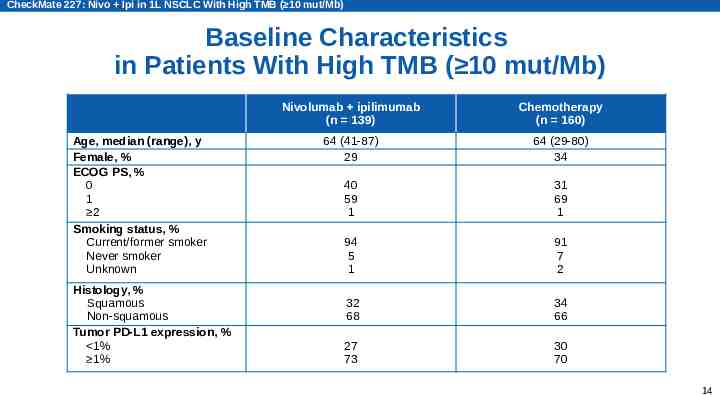
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Baseline Characteristics in Patients With High TMB ( 10 mut/Mb) Age, median (range), y Female, % ECOG PS, % 0 1 2 Smoking status, % Current/former smoker Never smoker Unknown Histology, % Squamous Non-squamous Tumor PD-L1 expression, % 1% 1% Nivolumab ipilimumab (n 139) Chemotherapy (n 160) 64 (41-87) 29 64 (29-80) 34 40 59 1 31 69 1 94 5 1 91 7 2 32 68 34 66 27 73 30 70 14
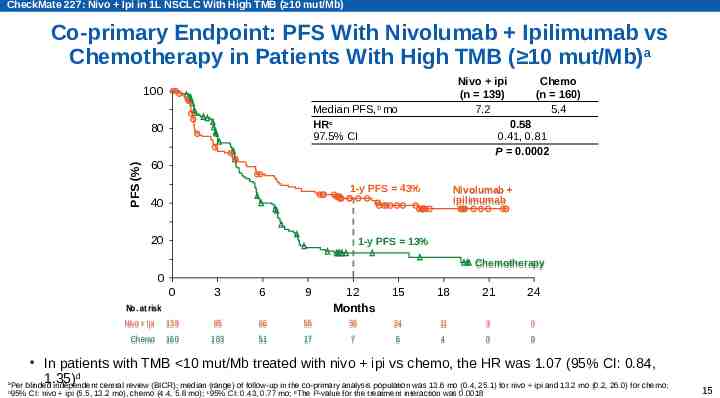
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Co-primary Endpoint: PFS With Nivolumab Ipilimumab vs Chemotherapy in Patients With High TMB ( 10 mut/Mb)a Nivo ipi (n 139) 7.2 100 Median PFS,b mo HRc 97.5% CI PFS (%) 80 Chemo (n 160) 5.4 0.58 0.41, 0.81 P 0.0002 60 1-y PFS 43% Nivolumab ipilimumab 40 20 1-y PFS 13% Chemotherapy 0 0 3 6 9 12 Months 15 18 21 24 Nivo Nivo ipi ipi 139 139 85 85 66 66 55 55 36 36 24 24 11 11 33 00 Chemo Chemo 160 160 103 103 51 51 17 17 77 66 44 00 00 No. at risk a b In patients with TMB 10 mut/Mb treated with nivo ipi vs chemo, the HR was 1.07 (95% CI: 0.84, 1.35)d Per blinded independent central review (BICR); median (range) of follow-up in the co-primary analysis population was 13.6 mo (0.4, 25.1) for nivo ipi and 13.2 mo (0.2, 26.0) for chemo; 95% CI: nivo ipi (5.5, 13.2 mo), chemo (4.4, 5.8 mo); c95% CI: 0.43, 0.77 mo; dThe P-value for the treatment interaction was 0.0018 15
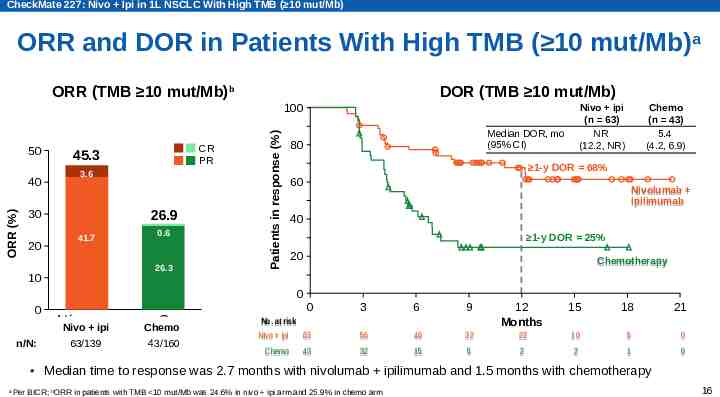
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) ORR and DOR in Patients With High TMB ( 10 mut/Mb) a ORR (TMB 10 mut/Mb)b DOR (TMB 10 mut/Mb) 50 ORR (%) 40 45.3 3.6 26.9 30 20 CR PR 41.7 0.6 26.3 10 Patients in response (%) 100 Nivo ipi (n 63) NR (12.2, NR) Median DOR, mo (95% CI) 80 Chemo (n 43) 5.4 (4.2, 6.9) 1-y DOR 68% 60 Nivolumab ipilimumab 40 1-y DOR 25% 20 Chemotherapy 0 0 n/N: Nivo Nivo . ipi C Chemo 63/139 43/160 0 3 6 9 15 18 21 No. No. at at risk risk Nivo ipi 63 Nivo ipi 63 12 Months 56 56 46 46 32 32 22 22 10 10 55 00 32 32 15 15 55 22 22 11 00 Chemo 43 43 Median time to response was 2.7 months with nivolumab ipilimumab and 1.5 months with chemotherapy a Per BICR; bORR in patients with TMB 10 mut/Mb was 24.6% in nivo ipi arm and 25.9% in chemo arm 16
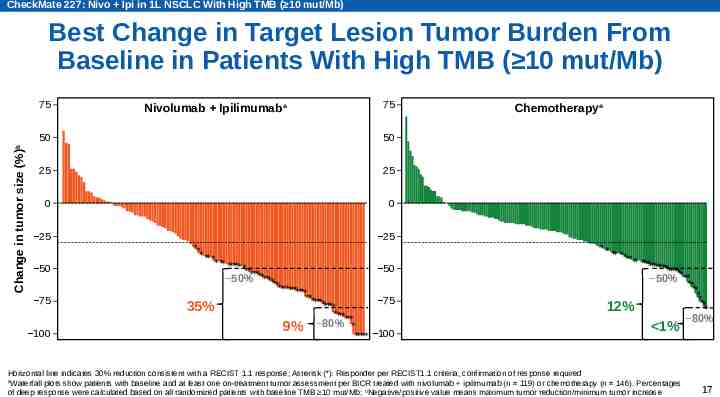
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Best Change in Target Lesion Tumor Burden From Baseline in Patients With High TMB ( 10 mut/Mb) Change in tumor size (%)b 75 Nivolumab Ipilimumaba 75 50 50 25 25 0 0 25 50 75 100 Chemotherapya 25 ** * ** * *** ***** *** 50 *** 50% ******* ***** ******* ****** 75 ***** 35% **** *** 9% 80% * 100 ***** ** ** ** **** ** ********** ******* 50% **** ** * ** ** 12% * 1% Horizontal line indicates 30% reduction consistent with a RECIST 1.1 response; Asterisk (*): Responder per RECIST1.1 criteria, confirmation of response required a Waterfall plots show patients with baseline and at least one on-treatment tumor assessment per BICR treated with nivolumab ipilimumab (n 119) or chemotherapy (n 146). Percentages of deep response were calculated based on all randomized patients with baseline TMB 10 mut/Mb; bNegative/positive value means maximum tumor reduction/minimum tumor increase 80% 17
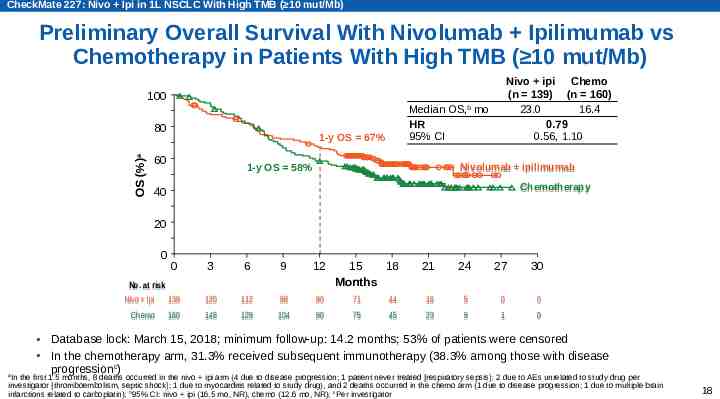
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Preliminary Overall Survival With Nivolumab Ipilimumab vs Chemotherapy in Patients With High TMB ( 10 mut/Mb) Nivo ipi Chemo (n 139) (n 160) 23.0 16.4 0.79 0.56, 1.10 100 OS (%)a 80 Median OS,b mo HR 95% CI 1-y OS 67% 60 Nivolumab ipilimumab 1-y OS 58% Chemotherapy 40 20 0 0 No. No. at at risk risk Nivo ipi 139 Chemo Chemo 160 3 6 9 12 15 18 Months 120 112 98 90 71 148 129 104 90 75 21 24 27 30 44 16 5 0 0 45 23 9 1 0 Database lock: March 15, 2018; minimum follow-up: 14.2 months; 53% of patients were censored In the chemotherapy arm, 31.3% received subsequent immunotherapy (38.3% among those with disease progressionc) In the first 1.5 months, 8 deaths occurred in the nivo ipi arm (4 due to disease progression; 1 patient never treated [respiratory sepsis]; 2 due to AEs unrelated to study drug per investigator [thromboembolism, septic shock]; 1 due to myocarditis related to study drug), and 2 deaths occurred in the chemo arm (1 due to disease progression; 1 due to multiple brain infarctions related to carboplatin); b95% CI: nivo ipi (16.5 mo, NR), chemo (12.6 mo, NR); cPer investigator a 18
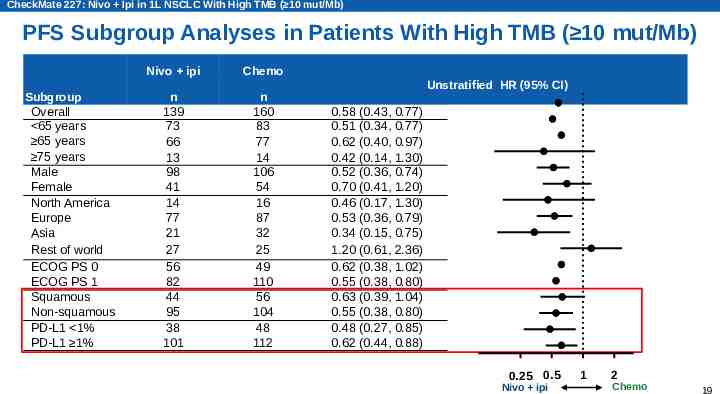
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) PFS Subgroup Analyses in Patients With High TMB ( 10 mut/Mb) Subgroup Overall 65 years 65 years 75 years Male Female North America Europe Asia Rest of world ECOG PS 0 ECOG PS 1 Squamous Non-squamous PD-L1 1% PD-L1 1% Nivo ipi Chemo n 139 73 66 13 98 41 14 77 21 27 56 82 44 95 38 101 n 160 83 77 14 106 54 16 87 32 25 49 110 56 104 48 112 Unstratified HR (95% CI) 0.58 (0.43, 0.77) 0.51 (0.34, 0.77) 0.62 (0.40, 0.97) 0.42 (0.14, 1.30) 0.52 (0.36, 0.74) 0.70 (0.41, 1.20) 0.46 (0.17, 1.30) 0.53 (0.36, 0.79) 0.34 (0.15, 0.75) 1.20 (0.61, 2.36) 0.62 (0.38, 1.02) 0.55 (0.38, 0.80) 0.63 (0.39, 1.04) 0.55 (0.38, 0.80) 0.48 (0.27, 0.85) 0.62 (0.44, 0.88) 0.25 0.5 Nivo ipi 1 2 Chemo 19
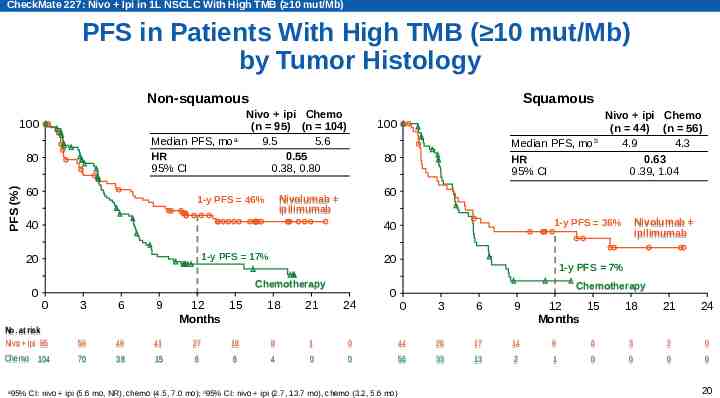
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) PFS in Patients With High TMB ( 10 mut/Mb) by Tumor Histology Non-squamous 100 Median PFS, moa HR 95% CI PFS (%) 80 60 Nivo ipi Chemo (n 95) (n 104) 9.5 5.6 0.55 0.38, 0.80 100 1-y PFS 17% 20 Chemotherapy 3 6 9 No. at risk 95 Nivo ipi 95 59 59 49 49 41 41 27 27 Chemo Chemo 70 38 15 6 104 12 15 Months 18 21 24 18 18 88 11 6 4 0 0 1-y PFS 7% Chemotherapy 0 3 6 9 00 44 44 26 26 17 17 14 14 99 0 56 33 13 2 1 95% CI: nivo ipi (5.6 mo, NR), chemo (4.5, 7.0 mo); b95% CI: nivo ipi (2.7, 13.7 mo), chemo (3.2, 5.6 mo) Nivolumab ipilimumab 1-y PFS 36% 40 0 Nivo ipi Chemo (n 44) (n 56) 4.9 4.3 0.63 0.39, 1.04 60 40 0 Median PFS, mob HR 95% CI 80 Nivolumab ipilimumab 1-y PFS 46% 20 a Squamous 12 15 Months 18 21 24 66 33 22 00 0 0 0 0 20
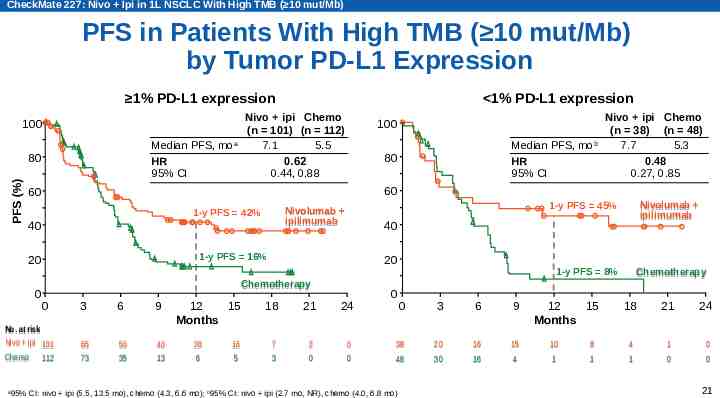
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) PFS in Patients With High TMB ( 10 mut/Mb) by Tumor PD-L1 Expression 1% PD-L1 expression 100 Median PFS, moa HR 95% CI PFS (%) 80 Nivo ipi Chemo (n 101) (n 112) 7.1 5.5 0.62 0.44, 0.88 100 40 1-y PFS 16% 20 Chemotherapy 0 No. No. at at risk risk Nivo ipi Nivo ipi 101 101 112 112 3 6 9 65 65 73 73 50 50 35 35 40 40 13 13 12 15 Months 26 26 66 16 16 55 Nivolumab ipilimumab 1-y PFS 45% Nivolumab ipilimumab 40 Chemo Nivo ipi Chemo (n 38) (n 48) 7.7 5.3 0.48 0.27, 0.85 60 1-y PFS 42% 0 Median PFS, mob HR 95% CI 80 60 20 a 1% PD-L1 expression 18 21 24 77 33 22 00 00 00 0 1-y PFS 8% 0 3 6 9 38 38 48 48 20 20 30 30 16 16 16 16 15 15 44 95% CI: nivo ipi (5.5, 13.5 mo), chemo (4.3, 6.6 mo); b95% CI: nivo ipi (2.7 mo, NR), chemo (4.0, 6.8 mo) 12 15 Months 10 10 11 88 11 Chemotherapy 18 21 24 44 11 11 00 00 00 21
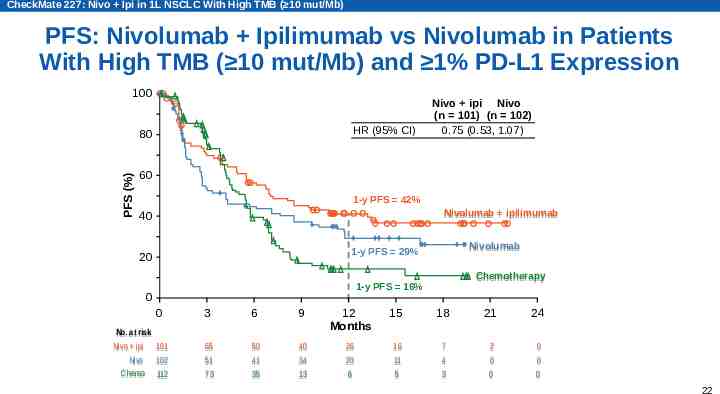
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) PFS: Nivolumab Ipilimumab vs Nivolumab in Patients With High TMB ( 10 mut/Mb) and 1% PD-L1 Expression 100 HR (95% CI) PFS (%) 80 Nivo ipi Nivo (n 101) (n 102) 0.75 (0.53, 1.07) 60 1-y PFS 42% Nivolumab ipilimumab 40 Nivolumab 1-y PFS 29% 20 Chemotherapy 1-y PFS 16% 0 0 No. at risk Nivo ipi 101 Nivo 102 Chemo 112 Chemo 112 3 6 9 12 Months 15 18 21 24 65 51 73 73 50 41 35 35 40 34 13 13 26 20 66 16 11 55 7 4 33 2 0 00 0 0 00 22
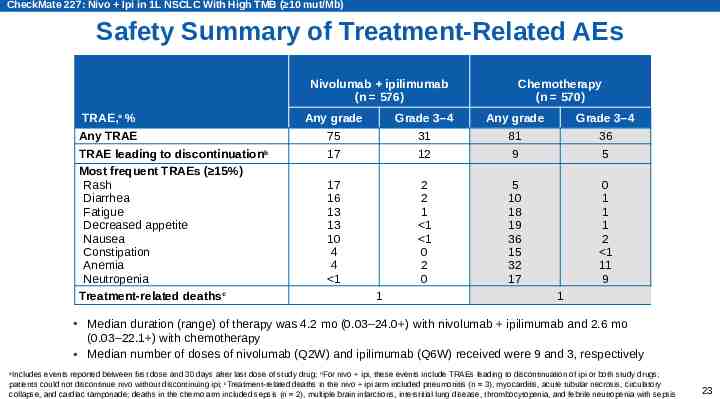
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Safety Summary of Treatment-Related AEs Nivolumab ipilimumab (n 576) TRAE,a % Any TRAE TRAE leading to discontinuationb Most frequent TRAEs ( 15%) Rash Diarrhea Fatigue Decreased appetite Nausea Constipation Anemia Neutropenia Treatment-related deathsc Chemotherapy (n 570) Any grade Grade 3–4 Any grade Grade 3–4 75 17 31 12 81 9 36 5 17 16 13 13 10 4 4 1 2 2 1 1 1 0 2 0 5 10 18 19 36 15 32 17 0 1 1 1 2 1 11 9 1 1 Median duration (range) of therapy was 4.2 mo (0.03–24.0 ) with nivolumab ipilimumab and 2.6 mo (0.03–22.1 ) with chemotherapy Median number of doses of nivolumab (Q2W) and ipilimumab (Q6W) received were 9 and 3, respectively Includes events reported between first dose and 30 days after last dose of study drug; bFor nivo ipi, these events include TRAEs leading to discontinuation of ipi or both study drugs; patients could not discontinue nivo without discontinuing ipi; cTreatment-related deaths in the nivo ipi arm included pneumonitis (n 3), myocarditis, acute tubular necrosis, circulatory collapse, and cardiac tamponade; deaths in the chemo arm included sepsis (n 2), multiple brain infarctions, interstitial lung disease, thrombocytopenia, and febrile neutropenia with sepsis a 23
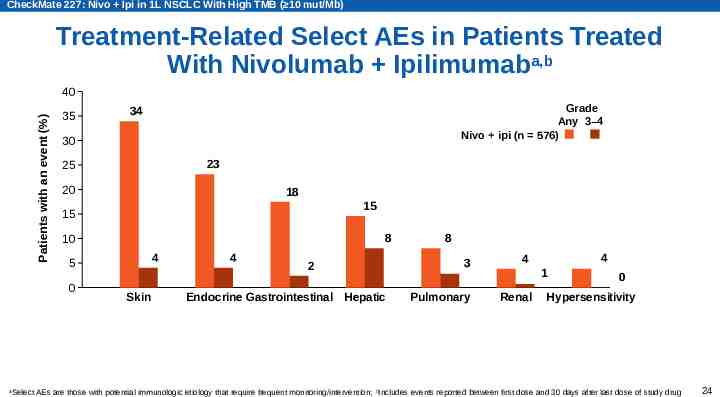
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Treatment-Related Select AEs in Patients Treated With Nivolumab Ipilimumaba,b Patients with an event (%) 40 35 30 23 25 20 18 15 15 8 10 4 5 0 a Grade Any 3–4 Nivo ipi (n 576) 34 Skin 4 2 Endocrine Gastrointestinal Hepatic 8 3 Pulmonary 4 4 1 Renal 0 Hypersensitivity Select AEs are those with potential immunologic etiology that require frequent monitoring/intervention; bIncludes events reported between first dose and 30 days after last dose of study drug 24
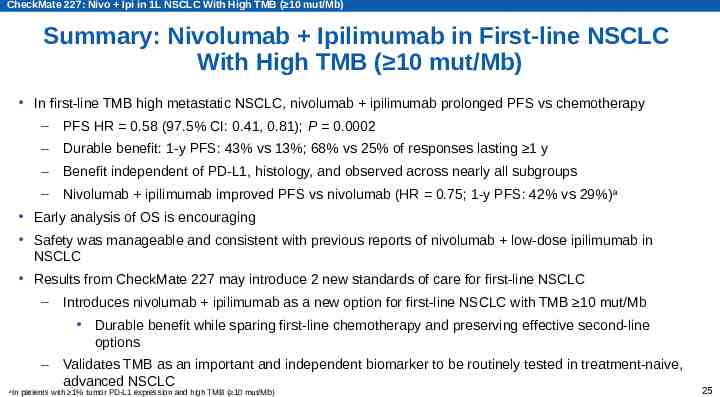
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Summary: Nivolumab Ipilimumab in First-line NSCLC With High TMB ( 10 mut/Mb) In first-line TMB high metastatic NSCLC, nivolumab ipilimumab prolonged PFS vs chemotherapy – PFS HR 0.58 (97.5% CI: 0.41, 0.81); P 0.0002 – Durable benefit: 1-y PFS: 43% vs 13%; 68% vs 25% of responses lasting 1 y – Benefit independent of PD-L1, histology, and observed across nearly all subgroups – Nivolumab ipilimumab improved PFS vs nivolumab (HR 0.75; 1-y PFS: 42% vs 29%) a Early analysis of OS is encouraging Safety was manageable and consistent with previous reports of nivolumab low-dose ipilimumab in NSCLC Results from CheckMate 227 may introduce 2 new standards of care for first-line NSCLC – Introduces nivolumab ipilimumab as a new option for first-line NSCLC with TMB 10 mut/Mb Durable benefit while sparing first-line chemotherapy and preserving effective second-line options – a Validates TMB as an important and independent biomarker to be routinely tested in treatment-naive, advanced NSCLC In patients with 1% tumor PD-L1 expression and high TMB ( 10 mut/Mb) 25
26
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227 Part 1 Investigators Argentina: S. Bella, C. Brocca, M. Flores, E. Korbenfeld, R. Kowalyszyn, L. Lupinacci, C. Martin, E. Richardet, MS. Varela, J. Zarba Greece: H. Linardou, P. Makrantonakis, D. Mavroudis, K. Syrigos Hungary: I. Albert, G. Losonczy, G. Ostoros Australia: M. Chan, K. Feeney, M. George, R. Joshi, A. Khattak, D. Leong, B. Markman, S-A. McLachlan, A. Nagrial, K. O’Byrne Ireland: O. Breathnach, L. Coate, S. Cuffe, P. Donnellan Austria: T. Fuereder, R. Kolb, H. Stoeger Israel: J. Bar, A. Cyjon, M. Gottfried, H. Nechushtan, S. Stemmer Belgium: B. Colinet, I. Demedts, K. Deschepper, V. Surmont, J. Van Meerbeeck Brazil: L. Araujo, C. Barrios, G. De Castro, F. Franke, C. Haddad, P. Marchi, C. Mathias, T. Oliveira Canada: J-S. Aucoin, V. Cohen, F. Couture, R. Lester, K. Marquis, S. Martel, M. Pavic, R. Sangha, M. Vincent Chile: O. Aren Frontera, P. Gonzalez Mella, P. Salman Colombia: R. Bruges, A. Cardona Zorrilla, A. Quiroga, G. Rojas Czech Republic: L. Havel, V. Kolek Finland: J. Koivunen, T. Saariaho France: C. Audigier-Valette, F. Barlesi, C. Chouaid, R. Corre, P. Fournel, R. Gervais, M. Ginoux, B. Mennecier, J. Raimbourg, L. Thiberville, R. Veillon, A. Vergnenegre, V. Westeel, G. Zalcman Germany: H. Bischoff, P. Fix, N. Frickhofen, W. Gleiber, C. Grohé, M. Kimmich, K. Kokowski, S. Lang, M. Reck, J. Schreiber, M. Schuler, C. Schumann, W. Schütte, M. Serke Italy: A. Ardizzoni, R. Bartolucci, L. Bonomi, F. Cappuzzo, R. Chiari, F. Cognetti, F. De Marinis, M. Garassino, C. Gridelli, E. Minenza Japan: K. Azuma, H. Daga, Y. Fujisaka, T. Fukuhara, K. Goto, M. Harada, A. Hata, T. Hida, K. Hotta, S. Ikeda, A. Inoue, Y. Iwamoto, K. Kasahara, I. Kinoshita, K. Kubota, T. Kurata, K. Minato, T. Naito, M. Nishio, N. Nogami, Y. Ohe, H. Okamoto, I. Okamoto, T. Okano, H. Saka, H. Sakai, M. Satouchi, S. Sugawara, M. Takeda, Y. Takiguchi, H. Tanaka, N. Yamamoto, T. Yokoyama Lebanon: M. Ghosn, A. Tfayli Mexico: J. Alatorre Alexander, F. Bustamante Valles, S. Campos Gomez, E. De la Mora Jimenez, P. Gonzalez, O. Hernandez Flores, F. Medina-Soto, M. Perez Martinez, J. Reyes Contreras, M. Segura Gonzalez, L. Vazquez Cortes Netherlands: J. Aerts, S. Burgers, R. Cornelissen, AJ. De Langen, M. Youssef-El Soud Peru: F. Hurtado De Mendoza, L. Mas, C. Vallejos Poland: E. Kalinka-Warzocha, K. Lesniewski-Kmak, I. Pawlak, A. Pluzanski, R. Suwinski, J. Wojcik-Tomaszewska, B. Zurawski Republic of Korea: J-H. Kang, S-W. Kim, JS. Lee, KH. Lee, K. Park Romania: A. Alexandru, T. Ciuleanu, M. Schenker, A. Ungureanu Russian Federation: O. Gladkov, N. Karaseva, K. Laktionov, A. Luft, V. Moiseyenko, G. Mukhametshina, D. Sakaeva South Africa: S. Chan, L. Dreosti, B. Rapoport, D. Rens Spain: R. Bernabe Caro, A. Blasco, E. Carcereny Costa, A. Martinez Marti, L. Paz-Ares, M. Provencio Switzerland: M. Mark, A. Mueller, S. Peters, S. Rothschild Taiwan: G-C. Chang, C-H. Chiu, K-Y. Lee, C-T. Yang, CJ. Yu United Kingdom: S. Ahmed, D. Chao, D. Gilligan, L. Li, M. Mackean, G. Middleton, C. Ottensmeier, S. Popat, J. Spicer United States: W. Akerley, S. Arledge, F. Badin, B. Bolemon, H. Borghaei, J. Brahmer, H. Chen, A. Dowlati, E. Gamboa, D. Gerber, S. Gettinger, M. Hellmann, L. Horn, A. Kramer, P. Lowry, D. Morgensztern, S. Nair, G. Otterson, R. Oyola, S. Ramalingam, R. Reilly, R. Siegel, J. Wrangle, R. Zinner 27
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Acknowledgments The patients and families who made this trial possible The clinical study teams who participated in the trial Suresh Alaparthy, Judith Bushong, and Christopher Coira (Bristol-Myers Squibb) for their contributions as protocol managers of this study and Haolan Lu (Bristol-Myers Squibb) for contributions to the statistical analysis plan Foundation Medicine for collaborative development of the FoundationOne CDx assay Dako for collaborative development of the automated PD-L1 IHC 28-8 pharmDx assay Bristol-Myers Squibb (Princeton, NJ) and ONO Pharmaceutical Company Ltd. (Osaka, Japan) All authors contributed to and approved the presentation; writing and editorial assistance was provided by Kerry K. Brinkman, PhD, of Evidence Scientific Solutions Inc, funded by Bristol-Myers Squibb 28
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Abbreviations 1L first-line AE adverse event AUC area under the curve BICR blinded independent central review Chemo chemotherapy CI confidence interval CR complete response DOR duration of response ECOG PS Eastern Cooperative Oncology Group performance status HR hazard ratio Ipi ipilimumab Mut mutation Nivo nivolumab NR not reached NSCLC non-small cell lung cancer NSQ non-squamous ORR objective response rate OS overall survival PD-L1 programmed death ligand 1 PFS progression-free survival PR partial response QC quality control Q2W every 2 weeks Q3W every 3 weeks Q6W every 6 weeks R randomized RCC renal cell carcinoma ROC receiver operating characteristic SCLC small cell lung cancer SQ squamous TMB tumor mutational burden TRAE treatment-related adverse event 29
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) Back-up 30
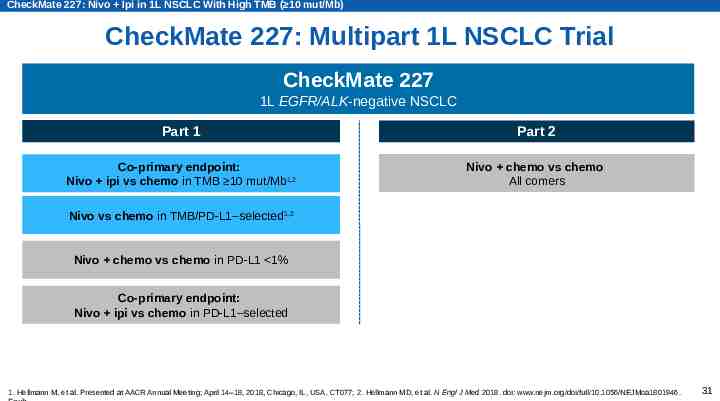
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227: Multipart 1L NSCLC Trial CheckMate 227 1L EGFR/ALK-negative NSCLC Part 1 Part 2 Co-primary endpoint: Nivo ipi vs chemo in TMB 10 mut/Mb1,2 Nivo chemo vs chemo All comers Nivo vs chemo in TMB/PD-L1–selected1,2 Nivo chemo vs chemo in PD-L1 1% Co-primary endpoint: Nivo ipi vs chemo in PD-L1–selected 1. Hellmann M, et al. Presented at AACR Annual Meeting; April 14–18, 2018, Chicago, IL, USA. CT077; 2. Hellmann MD, et al. N Engl J Med 2018. doi: www.nejm.org/doi/full/10.1056/NEJMoa1801946. 31
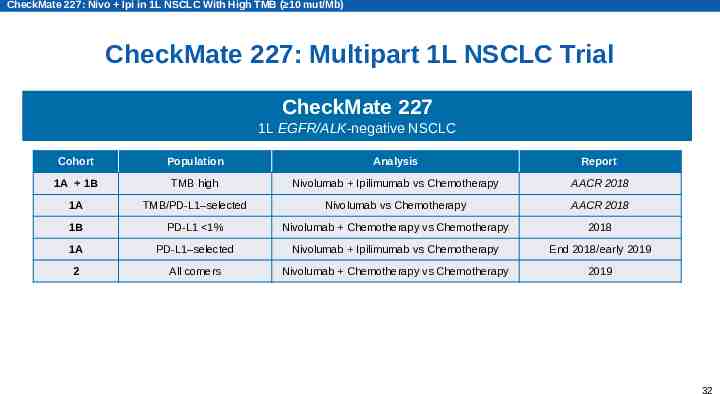
CheckMate 227: Nivo Ipi in 1L NSCLC With High TMB ( 10 mut/Mb) CheckMate 227: Multipart 1L NSCLC Trial CheckMate 227 1L EGFR/ALK-negative NSCLC Cohort Population Analysis Report 1A 1B TMB high Nivolumab Ipilimumab vs Chemotherapy AACR 2018 1A TMB/PD-L1–selected Nivolumab vs Chemotherapy AACR 2018 1B PD-L1 1% Nivolumab Chemotherapy vs Chemotherapy 2018 1A PD-L1–selected Nivolumab Ipilimumab vs Chemotherapy End 2018/early 2019 2 All comers Nivolumab Chemotherapy vs Chemotherapy 2019 32
CheckMate 568 CT078 2018 CHICAGO, IL Tumor Mutational Burden (TMB) as a Biomarker for Clinical Benefit From Dual Immune Checkpoint Blockade With Nivolumab Ipilimumab in First-line Non-Small Cell Lung Cancer: Identification of TMB Cutoff From CheckMate 568 Suresh S. Ramalingam,1 Matthew D. Hellmann,2 Mark M. Awad,3 Hossein Borghaei,4 Justin Gainor,5 Julie Brahmer,6 David R. Spigel,7 Martin Reck,8 Kenneth J. O’Byrne,9 Luis Paz-Ares,10 Kim Zerba,11 Xuemei Li,11 William J. Geese,11 George Green,11 Brian Lestini,11 Joseph D. Szustakowski,11 Han Chang,11 Neal Ready12 Winship Cancer Institute, Emory University, Atlanta, GA, USA; 2Memorial Sloan Kettering Cancer Center, New York, NY, USA; 3 Dana-Farber Cancer Institute, Boston, MA, USA; 4Fox Chase Cancer Center, Philadelphia, PA, USA; 5Massachusetts General Hospital, Boston, MA, USA; 6Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA; 7Sarah Cannon Research Institute, Nashville, TN, USA; 8Lung Clinic Grosshansdorf, Airway Research Center North (ARCN), member of the German Center for Lung Research (DZL), Grosshansdorf, Germany; 9Princess Alexandra Hospital, Brisbane, Queensland, Australia; 10Hospital Universitario Doce de Octubre, CNIO, Universidad Complutense & CiberOnc, Madrid, Spain; 11Bristol-Myers Squibb, Princeton, NJ, USA; 12Duke University Medical Center, Durham, NC, USA 1 ID 1506IT18NP01399-01
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Introduction Approved approaches in 1L NSCLC include anti–PD-1 monotherapy in patients with 50% tumor PD-L1 expression and I-O combined with chemotherapy Despite recent advances, there remains an unmet need for biomarkers that identify patients more likely to benefit from I-O therapies Nivolumab ipilimumab demonstrated durable clinical activity in 1L NSCLC in the CheckMate 012 trial1,2 – Dosing of nivolumab 3 mg/kg Q2W ipilimumab 1 mg/kg Q6W was optimized for NSCLC (13% discontinuation due to TRAEs in nivolumab low-dose ipilimumab) TMB is an emerging, predictive biomarker of response to I-O therapy in multiple tumor types, including lung cancer3-5 1. Hellmann MD, et al. Lancet Oncol 2017;18:31-41; 2. Goldman JW, et al. Poster presentation at ASCO 2017 Annual Meeting; June 2–6, 2017; Chicago, IL, USA. Abstract 9093; 3. Yarchoan M, et al. N Engl J Med 2017;377:2500-1; 4. Rizvi H, et al. J Clin Oncol 2018;36:633-41; 5. Hellmann MD, et al. Cancer Cell 2018. doi: https://doi.org/10.1016/j.ccell.2018.03.018. Epub 34
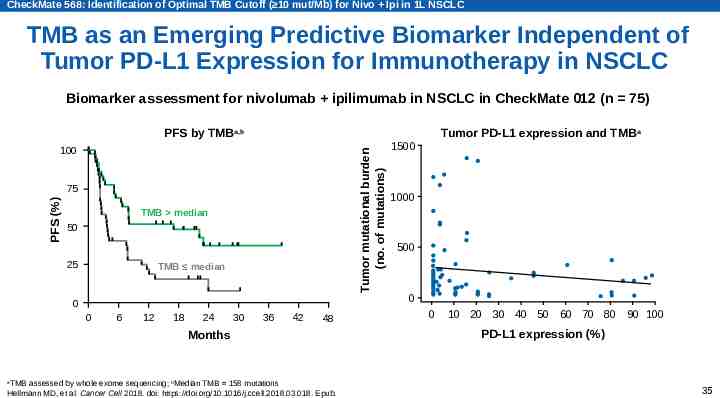
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC TMB as an Emerging Predictive Biomarker Independent of Tumor PD-L1 Expression for Immunotherapy in NSCLC Biomarker assessment for nivolumab ipilimumab in NSCLC in CheckMate 012 (n 75) PFS by TMBa,b Tumor mutational burden (no. of mutations) 100 PFS (%) 75 TMB median 50 25 TMB median 0 0 6 12 18 24 30 36 42 48 Months TMB assessed by whole exome sequencing; bMedian TMB 158 mutations Hellmann MD, et al. Cancer Cell 2018. doi: https://doi.org/10.1016/j.ccell.2018.03.018. Epub. Tumor PD-L1 expression and TMB a 1500 1000 500 0 0 10 20 30 40 50 60 70 80 90 100 PD-L1 expression (%) a 35
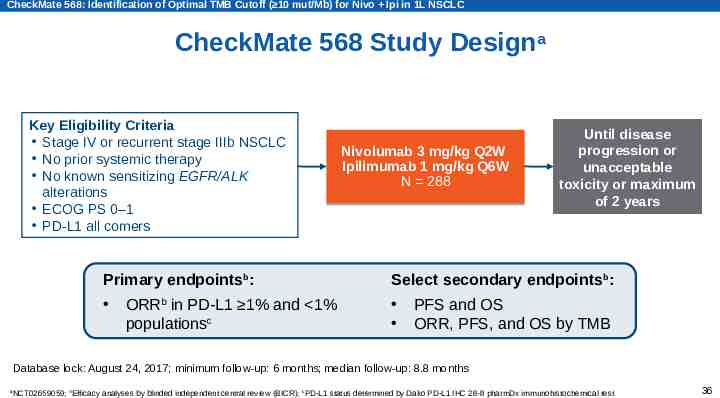
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC CheckMate 568 Study Designa Key Eligibility Criteria Stage IV or recurrent stage IIIb NSCLC No prior systemic therapy No known sensitizing EGFR/ALK alterations ECOG PS 0–1 PD-L1 all comers Nivolumab 3 mg/kg Q2W Ipilimumab 1 mg/kg Q6W N 288 Until disease progression or unacceptable toxicity or maximum of 2 years Primary endpointsb: Select secondary endpointsb: ORRb in PD-L1 1% and 1% populationsc PFS and OS ORR, PFS, and OS by TMB Database lock: August 24, 2017; minimum follow-up: 6 months; median follow-up: 8.8 months a NCT02659059; bEfficacy analyses by blinded independent central review (BICR); cPD-L1 status determined by Dako PD-L1 IHC 28-8 pharmDx immunohistochemical test 36
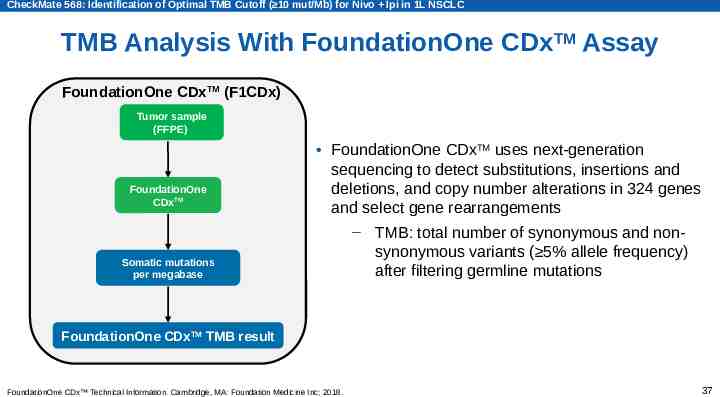
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC TMB Analysis With FoundationOne CDxTM Assay FoundationOne CDxTM (F1CDx) Tumor sample (FFPE) FoundationOne CDxTM FoundationOne CDxTM uses next-generation sequencing to detect substitutions, insertions and deletions, and copy number alterations in 324 genes and select gene rearrangements Somatic mutations per megabase – TMB: total number of synonymous and nonsynonymous variants ( 5% allele frequency) after filtering germline mutations FoundationOne CDxTM TMB result FoundationOne CDx Technical Information. Cambridge, MA: Foundation Medicine Inc; 2018. 37
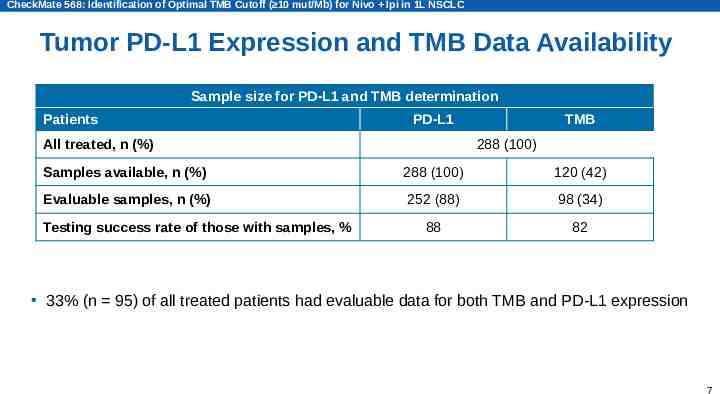
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Tumor PD-L1 Expression and TMB Data Availability Sample size for PD-L1 and TMB determination Patients PD-L1 All treated, n (%) TMB 288 (100) Samples available, n (%) 288 (100) 120 (42) Evaluable samples, n (%) 252 (88) 98 (34) 88 82 Testing success rate of those with samples, % 33% (n 95) of all treated patients had evaluable data for both TMB and PD-L1 expression 7
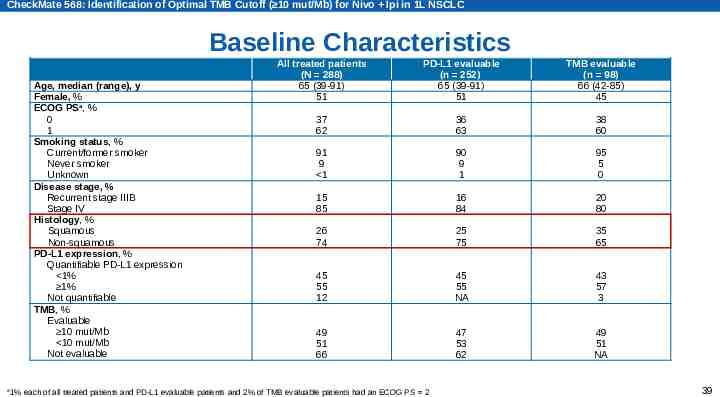
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Baseline Characteristics Age, median (range), y Female, % ECOG PSa, % 0 1 Smoking status, % Current/former smoker Never smoker Unknown Disease stage, % Recurrent stage IIIB Stage IV Histology, % Squamous Non-squamous PD-L1 expression, % Quantifiable PD-L1 expression 1% 1% Not quantifiable TMB, % Evaluable 10 mut/Mb 10 mut/Mb Not evaluable a All treated patients (N 288) 65 (39-91) 51 PD-L1 evaluable (n 252) 65 (39-91) 51 TMB evaluable (n 98) 66 (42-85) 45 37 62 36 63 38 60 91 9 1 90 9 1 95 5 0 15 85 16 84 20 80 26 74 25 75 35 65 45 55 12 45 55 NA 43 57 3 49 51 66 47 53 62 49 51 NA 1% each of all treated patients and PD-L1 evaluable patients and 2% of TMB evaluable patients had an ECOG PS 2 39
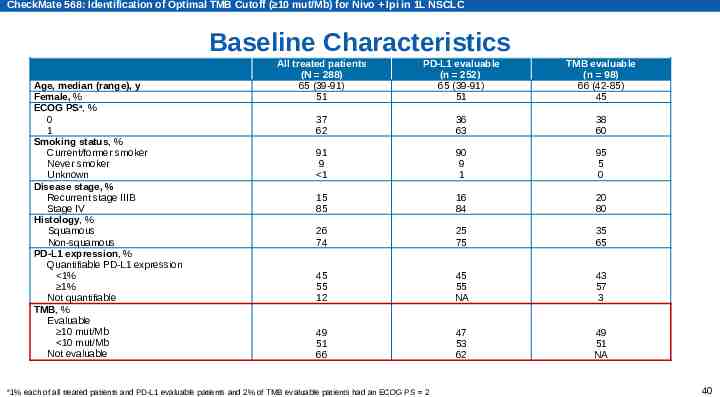
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Baseline Characteristics Age, median (range), y Female, % ECOG PSa, % 0 1 Smoking status, % Current/former smoker Never smoker Unknown Disease stage, % Recurrent stage IIIB Stage IV Histology, % Squamous Non-squamous PD-L1 expression, % Quantifiable PD-L1 expression 1% 1% Not quantifiable TMB, % Evaluable 10 mut/Mb 10 mut/Mb Not evaluable a All treated patients (N 288) 65 (39-91) 51 PD-L1 evaluable (n 252) 65 (39-91) 51 TMB evaluable (n 98) 66 (42-85) 45 37 62 36 63 38 60 91 9 1 90 9 1 95 5 0 15 85 16 84 20 80 26 74 25 75 35 65 45 55 12 45 55 NA 43 57 3 49 51 66 47 53 62 49 51 NA 1% each of all treated patients and PD-L1 evaluable patients and 2% of TMB evaluable patients had an ECOG PS 2 40
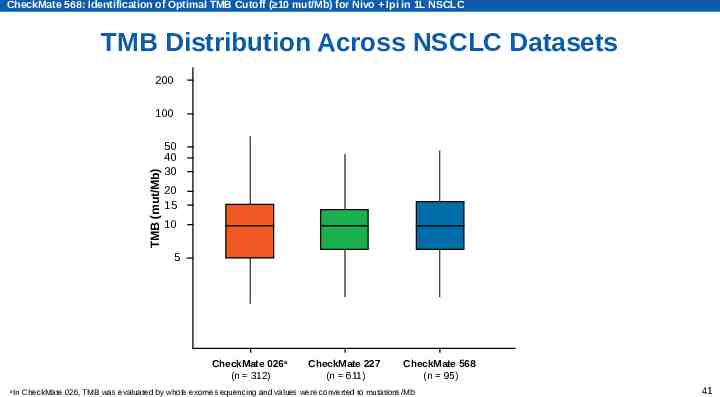
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC TMB Distribution Across NSCLC Datasets 200 TMB (mut/Mb) 100 50 40 30 20 15 10 5 CheckMate 026a (n 312) a CheckMate 227 (n 611) CheckMate 568 (n 95) In CheckMate 026, TMB was evaluated by whole exome sequencing and values were converted to mutations/Mb 41
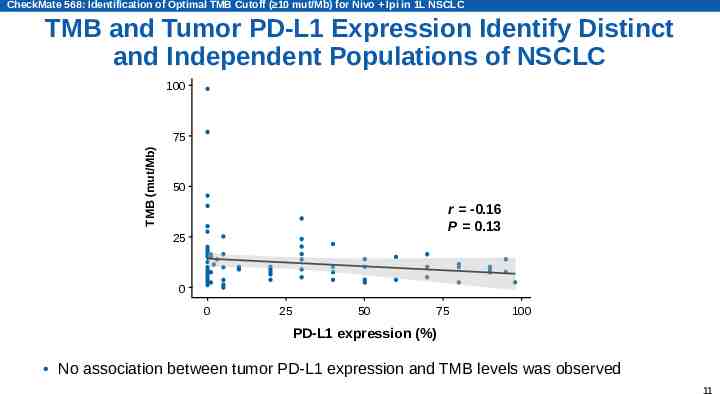
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC TMB and Tumor PD-L1 Expression Identify Distinct and Independent Populations of NSCLC 100 TMB (mut/Mb) 75 50 r -0.16 P 0.13 25 0 0 25 50 75 100 PD-L1 expression (%) No association between tumor PD-L1 expression and TMB levels was observed 11
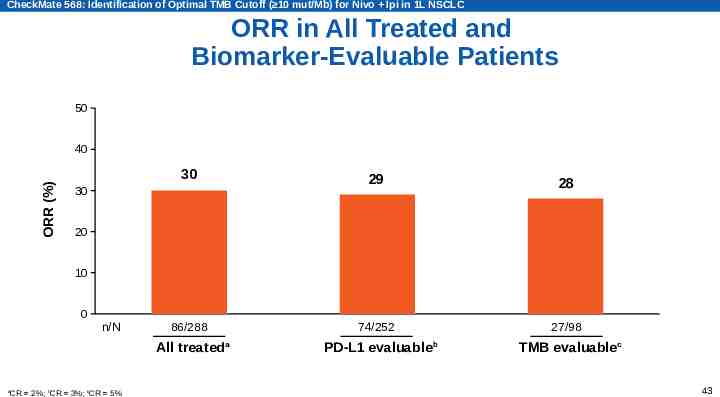
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC ORR in All Treated and Biomarker-Evaluable Patients 50 ORR (%) 40 30 29 28 86/288 74/252 27/98 30 20 10 0 n/N All treateda a CR 2%; bCR 3%; cCR 5% PD-L1 evaluableb TMB evaluablec 43
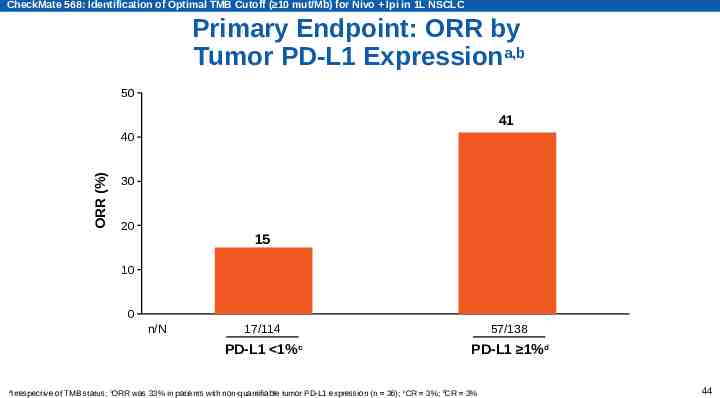
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Primary Endpoint: ORR by Tumor PD-L1 Expressiona,b 50 41 ORR (%) 40 30 3 20 15 3 10 0 n/N a 17/114 57/138 PD-L1 1%c PD-L1 1%d Irrespective of TMB status; bORR was 33% in patients with non-quantifiable tumor PD-L1 expression (n 36); cCR 3%; dCR 3% 44
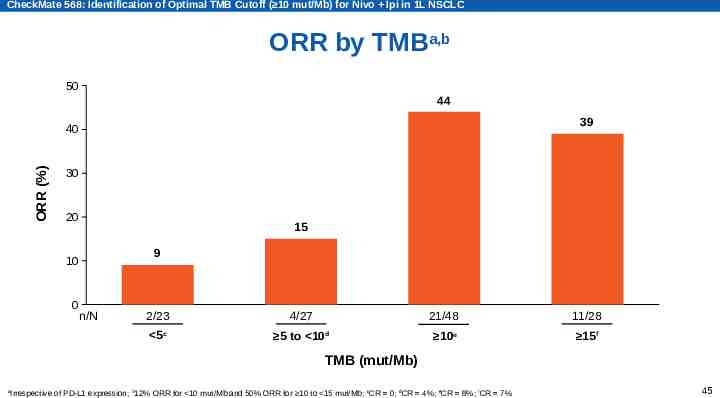
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC ORR by TMBa,b 50 44 39 ORR (%) 40 30 20 15 9 10 0 n/N 2/23 4/27 21/48 11/28 5c 5 to 10d 10e 15f TMB (mut/Mb) a Irrespective of PD-L1 expression; b12% ORR for 10 mut/Mb and 50% ORR for 10 to 15 mut/Mb; cCR 0; dCR 4%; eCR 8%; fCR 7% 45
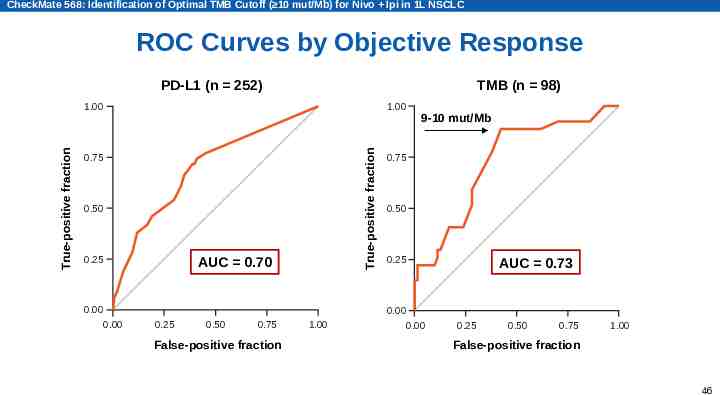
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC ROC Curves by Objective Response PD-L1 (n 252) TMB (n 98) 1.00 True-positive fraction True-positive fraction 1.00 0.75 0.50 0.25 AUC 0.70 0.00 0.00 0.25 0.50 0.75 False-positive fraction 1.00 9-10 mut/Mb 0.75 0.50 0.25 0.00 0.00 AUC 0.73 0.25 0.50 0.75 1.00 False-positive fraction 46
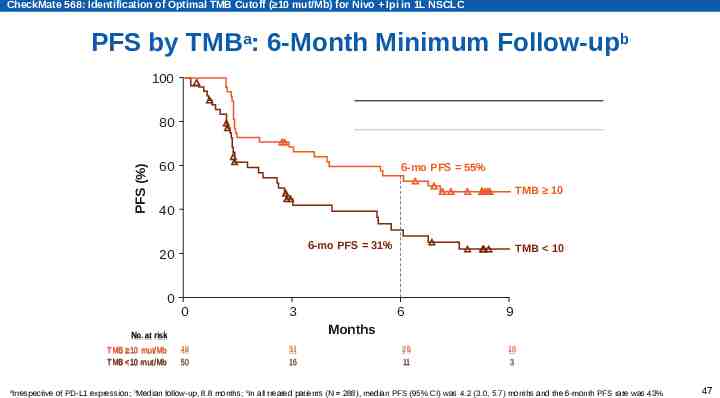
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC PFS by TMBa: 6-Month Minimum Follow-upb 100 Median PFS,c mo (95% CI) PFS (%) 80 60 TMB 10 mut/Mb (n 50) 7.1 (3.6, 11.3) 2.6 (1.4, 5.4) 6-mo PFS 55% TMB 10 40 6-mo PFS 31% 20 0 No. No. at at risk risk TMB 10 mut/Mb TMB 10 mut/Mb a TMB 10 mut/Mb (n 48) 0 3 TMB 10 6 9 Months 48 48 50 50 31 31 16 16 25 25 11 11 10 10 33 Irrespective of PD-L1 expression; bMedian follow-up, 8.8 months; cIn all treated patients (N 288), median PFS (95% CI) was 4.2 (3.0, 5.7) months and the 6-month PFS rate was 43% 47
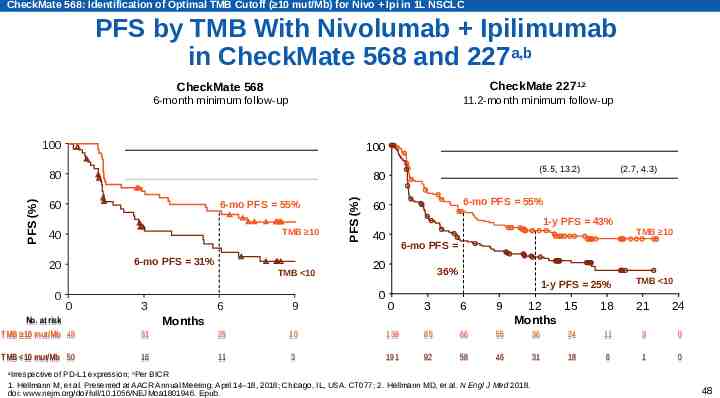
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC PFS by TMB With Nivolumab Ipilimumab in CheckMate 568 and 227a,b CheckMate 2271,2 CheckMate 568 11.2-month minimum follow-up 6-month minimum follow-up Median PFS, mo (95% CI) PFS (%) 80 TMB 10 mut/Mb (n 50) 7.1 (3.6, 11.3) 2.6 (1.4, 5.4) 6-mo PFS 55% 60 TMB 10 40 6-mo PFS 31% 20 0 TMB 10 0 No. No. at at risk risk 48 TMB 10 mut/Mb mut/Mb 48 TMB 10 TMB TMB 10 10 mut/Mb mut/Mb 50 3 TMB 10 mut/Mb (n 139) TMB 10 mut/Mb (n 191) 7.2 (5.5, 13.2) 3.2 (2.7, 4.3) 100 Median PFS, mo (95% CI) 80 PFS (%) 100 TMB 10 mut/Mb (n 48) 6-mo PFS 55% 60 1-y PFS 43% 40 6-mo PFS 20 0 36% 1-y PFS 25% 0 3 6 9 10 10 139 85 66 55 36 3 191 92 58 46 31 6 9 31 31 25 25 16 11 TMB 10 Months 12 15 Months Irrespective of PD-L1 expression; bPer BICR 1. Hellmann M, et al. Presented at AACR Annual Meeting; April 14–18, 2018; Chicago, IL, USA. CT077; 2. Hellmann MD, et al. N Engl J Med 2018. doi: www.nejm.org/doi/full/10.1056/NEJMoa1801946. Epub. TMB 10 18 21 24 24 11 3 0 18 6 1 0 a 48
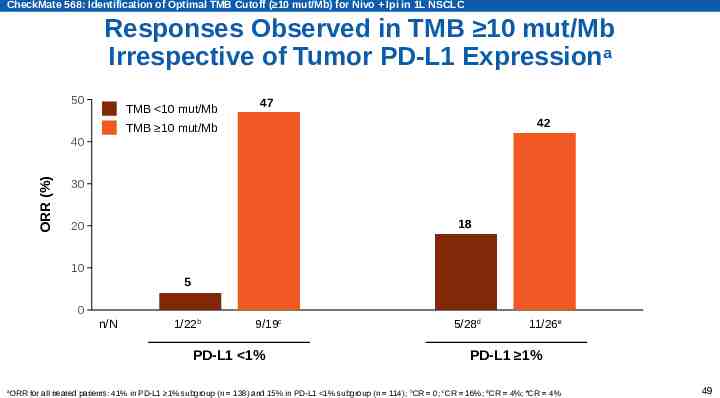
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Responses Observed in TMB 10 mut/Mb Irrespective of Tumor PD-L1 Expressiona 50 TMB 10 mut/Mb 47 42 TMB 10 mut/Mb ORR (%) 40 30 18 20 10 5 0 n/N 1/22b 9/19c PD-L1 1% a 5/28d 11/26e PD-L1 1% ORR for all treated patients: 41% in PD-L1 1% subgroup (n 138) and 15% in PD-L1 1% subgroup (n 114); bCR 0; cCR 16%; dCR 4%; eCR 4% 49
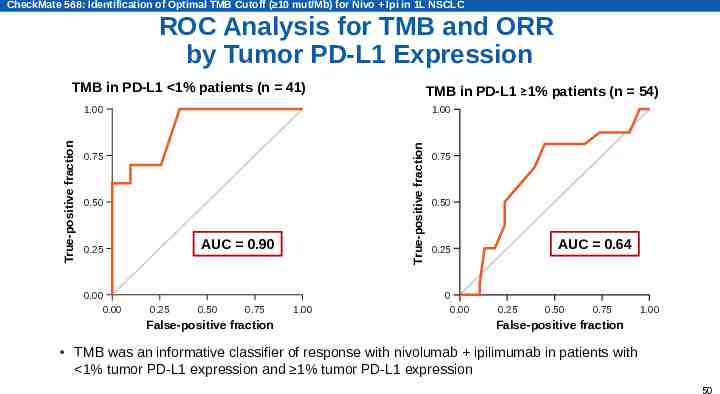
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC ROC Analysis for TMB and ORR by Tumor PD-L1 Expression TMB in PD-L1 1% patients (n 41) TMB in PD-L1 1% patients (n 54) 1.00 True-positive fraction True-positive fraction 1.00 0.75 0.50 AUC 0.90 0.25 0.00 0.00 0.25 0.50 0.75 False-positive fraction 1.00 0.75 0.50 AUC 0.64 0.25 0 0.00 0.25 0.50 0.75 1.00 False-positive fraction TMB was an informative classifier of response with nivolumab ipilimumab in patients with 1% tumor PD-L1 expression and 1% tumor PD-L1 expression 50
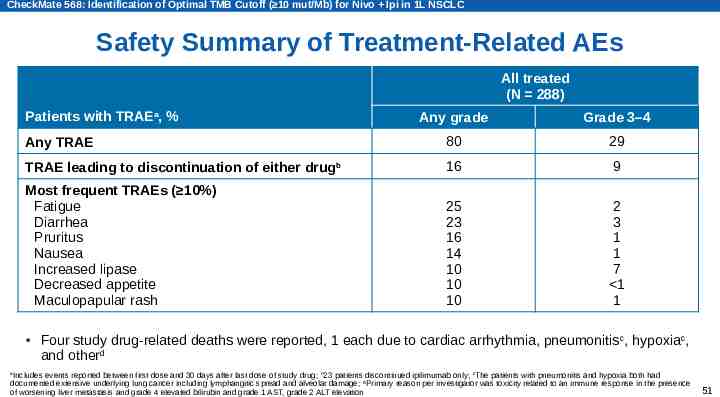
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Safety Summary of Treatment-Related AEs All treated (N 288) Patients with TRAEa, % Any grade Grade 3–4 Any TRAE 80 29 TRAE leading to discontinuation of either drugb 16 9 Most frequent TRAEs ( 10%) Fatigue Diarrhea Pruritus Nausea Increased lipase Decreased appetite Maculopapular rash 25 23 16 14 10 10 10 2 3 1 1 7 1 1 Four study drug-related deaths were reported, 1 each due to cardiac arrhythmia, pneumonitis c, hypoxiac, and otherd Includes events reported between first dose and 30 days after last dose of study drug; b23 patients discontinued ipilimumab only; cThe patients with pneumonitis and hypoxia both had documented extensive underlying lung cancer including lymphangitic spread and alveolar damage; dPrimary reason per investigator was toxicity related to an immune response in the presence of worsening liver metastasis and grade 4 elevated bilirubin and grade 1 AST, grade 2 ALT elevation a 51
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Treatment-Related Select AEsa,b All treated (N 288) Patients, % a Any grade Grade 3–4 Skin 30 3 Gastrointestinal 25 5 Endocrine 19 2 Hepatic 12 4 Hypersensitivity/infusion reaction 7 1 Pulmonary 7 2 Renal 1 1 Select AEs are those with potential immunologic etiology that require frequent monitoring/intervention; bIncludes events reported between first dose and 30 days after last dose of study drug 52
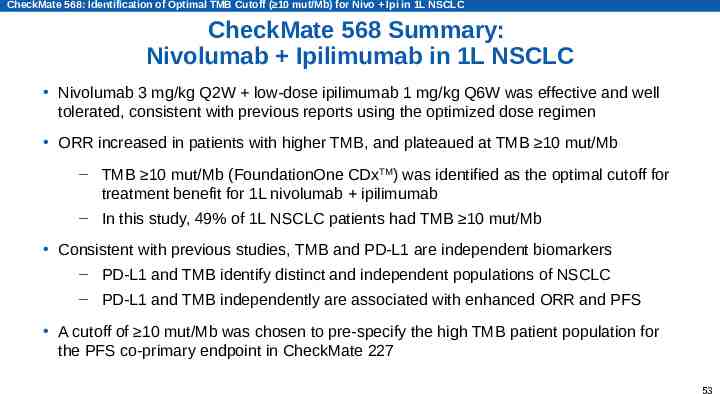
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC CheckMate 568 Summary: Nivolumab Ipilimumab in 1L NSCLC Nivolumab 3 mg/kg Q2W low-dose ipilimumab 1 mg/kg Q6W was effective and well tolerated, consistent with previous reports using the optimized dose regimen ORR increased in patients with higher TMB, and plateaued at TMB 10 mut/Mb – TMB 10 mut/Mb (FoundationOne CDxTM) was identified as the optimal cutoff for treatment benefit for 1L nivolumab ipilimumab – In this study, 49% of 1L NSCLC patients had TMB 10 mut/Mb Consistent with previous studies, TMB and PD-L1 are independent biomarkers – PD-L1 and TMB identify distinct and independent populations of NSCLC – PD-L1 and TMB independently are associated with enhanced ORR and PFS A cutoff of 10 mut/Mb was chosen to pre-specify the high TMB patient population for the PFS co-primary endpoint in CheckMate 227 53
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC CheckMate 568 Investigators United States: E. Avery, B. Bastos, H. Borghaei, Y. Boumber, J. Brahmer, B. Byrne, F. Chen, J. Chesney, S. Dakhil, G. Finley, J. Gainor, L. Gandhi, M. Gutierrez, M. Hellmann, L. Horn, J. Jolivet, J. Orcutt, G. Otterson, S. Ramalingam, N. Ready, O. Rixe, I. Rybkin, J. Schneider, S. Spadafora, D. Spigel, M. Taylor, A. Tomiak, K. Zu 54
CheckMate 568: Identification of Optimal TMB Cutoff ( 10 mut/Mb) for Nivo Ipi in 1L NSCLC Acknowledgments The patients and families who made this trial possible The clinical study teams who participated in the trial The protocol managers for this study, Jessica Proszynski and Katleen Van Hoefs, and Wenhua Hu for contributions for statistical analyses Foundation Medicine for collaborative development of FoundationOne CDx assay Dako for collaborative development of the automated PD-L1 IHC 28-8 pharmDx assay Bristol-Myers Squibb (Princeton, NJ) and ONO Pharmaceutical Company Ltd. (Osaka, Japan) All authors contributed to and approved the presentation; writing and editorial assistance was provided by Kerry K. Brinkman, PhD, and Leah Bernstein, PhD, of Evidence Scientific Solutions Inc, funded by Bristol-Myers Squibb 55
Abbreviations 1L first-line AE adverse event ALK anaplastic lymphoma kinase ALT alanine aminotransferase AST aspartate transaminase AUC area under the curve CI confidence interval CR complete response ECOG PS Eastern Cooperative Oncology Group performance status EGFR epidermal growth factor receptor I-O immuno-oncology Mut mutation NA not applicable NSCLC non-small cell lung cancer ORR objective response rate OS overall survival PD-1 programmed death-1 PD-L1 programmed death ligand 1 PFS progression-free survival Q2W every 2 weeks Q6W every 6 weeks ROC receiver operating characteristic TRAE treatment-related adverse event TMB tumor mutational burden 56