The evidence-base of treatment for heroin addiction: reducing drug

24 Slides782.50 KB
The evidence-base of treatment for heroin addiction: reducing drug problems, HIV and AIDS, and crime Professor John Strang National Addiction Centre, London, UK
‘Drug Policy and the Public Good’ The importance of treatment of heroin addiction Evidence-base of effectiveness of OST The ‘Recovery’ debate
Drug Policy and the Public Good Sponsored by: The Society for the Study of Addiction (UK) The Pan American Health Organization Other SSA books: Alcohol Policy and the Public Good (1994) Alcohol: No Ordinary Commodity (2003, 2010)
The Drugs and Public Policy Group (our ‘invisible college’) Co-authors Academic Affiliations John Strang National Addiction Centre (UK) Ingeborg Rossow Nat Inst Alcohol & Drug Research (Norway) Robin Room University of Melbourne (Australia) Peter Reuter University of Maryland (USA) Jürgen Rehm University of Toronto (Canada) Isidore Obot University of Uyo (Nigeria) Keith Humphreys Stanford University (USA) David Foxcroft Oxford Brookes University (UK) Benedikt Fischer Simon Fraser University (Canada) Griffith Edwards National Addiction Centre (UK) Jonathan Caulkins Carnagie Mellon University (USA) Thomas Babor University of Connecticut (USA)
The 4 false dichotomies Law enforcement ‘versus’ treatment (‘cops versus docs’) Abstinence ‘versus’ harm reduction Mistakenly presented as either/or ‘legal’ ‘versus’ ‘illegal’ drugs (‘good drugs’ versus ‘bad drugs’) ‘drug users’ ‘versus’ ‘mainstream society’ (overlapping; and health and social and c.j. gain for all)
For every complex problem, there is an answer H.L. Mencken
For every complex problem, there is an answer that is clear and simple H.L. Mencken
For every complex problem, there is an answer that is clear and simple and wrong H.L. Mencken
Purpose/objectives Methods/tools Measures/evaluation Process
‘Treatment works’ (Sorry, You can’t borrow efficacy) Surgery works Some conditions with no special Rx Variability in quality
‘I already know what works’ Dangerous arrogance much of Rx (almost certainly) padding disproportionate influence of advertising obscures clear support for effective . concentrate on proved quality marks
‘We can’t afford to do research’ Research for research’s sake Research for science’s sake Research for treatment’s sake
Quality of evidence I. Evidence obtained from at least one properly designed randomised controlled trial. II. - 1 well-designed controlled trials (not RCT). II. - 2 cohort or case-controlled analytical centre/group). studies (pref. 1 II. - 3 multiple time series with/without intervention. III. Opinions of respected authorities, based on clinical experience/descriptive studies, or reports of expert committees.
Types of Evidence Randomized clinical trials Descriptive epidemiology Quasi-experimental/correlational studies Natural experiments Qualitative research Health services research Historical research
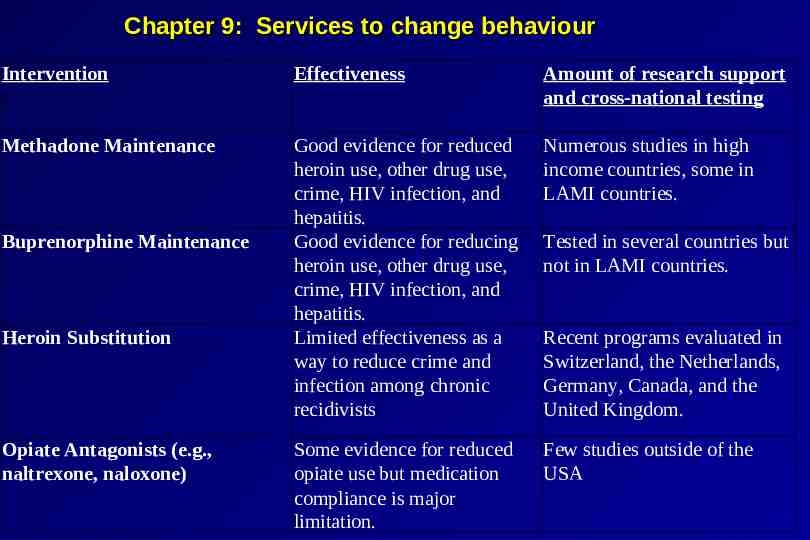
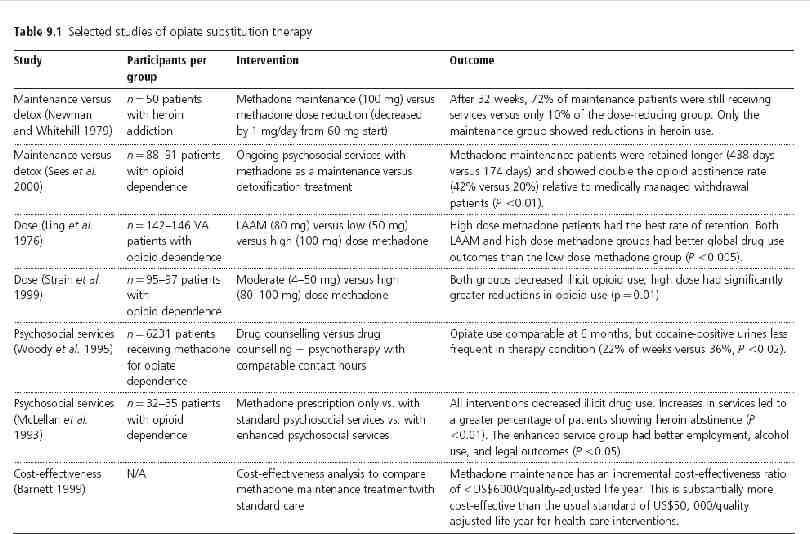
Chapter 9: Services to change behaviour Intervention Effectiveness Amount of research support and cross-national testing Methadone Maintenance Good evidence for reduced heroin use, other drug use, crime, HIV infection, and hepatitis. Good evidence for reducing heroin use, other drug use, crime, HIV infection, and hepatitis. Limited effectiveness as a way to reduce crime and infection among chronic recidivists Numerous studies in high income countries, some in LAMI countries. Some evidence for reduced opiate use but medication compliance is major limitation. Few studies outside of the USA Buprenorphine Maintenance Heroin Substitution Opiate Antagonists (e.g., naltrexone, naloxone) Tested in several countries but not in LAMI countries. Recent programs evaluated in Switzerland, the Netherlands, Germany, Canada, and the United Kingdom.
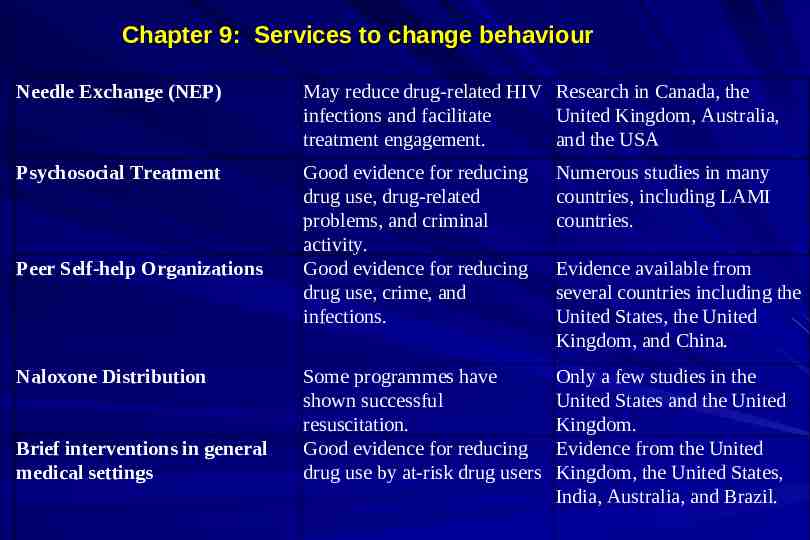
Chapter 9: Services to change behaviour Needle Exchange (NEP) May reduce drug-related HIV Research in Canada, the infections and facilitate United Kingdom, Australia, treatment engagement. and the USA Psychosocial Treatment Good evidence for reducing drug use, drug-related problems, and criminal activity. Good evidence for reducing drug use, crime, and infections. Numerous studies in many countries, including LAMI countries. Some programmes have shown successful resuscitation. Good evidence for reducing drug use by at-risk drug users Only a few studies in the United States and the United Kingdom. Evidence from the United Kingdom, the United States, India, Australia, and Brazil. Peer Self-help Organizations Naloxone Distribution Brief interventions in general medical settings Evidence available from several countries including the United States, the United Kingdom, and China.
Three service system changes that made a difference 1. Introduction of large scale opiate substitution services in France and Switzerland. 2. Creation of the drug court system in the United States. 3. Promotion of clinical practice guidelines for opiate substitution in the United Kingdom.
Treatment and Harm Minimization Services for opiate dependent individuals have the strongest supporting evidence; and they are also effective ways to reduce drug-related crime and the spread of HIV infection. Some harm reduction programs, such as needle exchange programs, reduce high risk injection practices and engage IDUs in treatment and health services.
Where services are sited in different countries Specialized drug and alcohol services Psychiatric care The general medical care system, including primary health care, general hospitals and teaching hospitals. The criminal justice/prison system. The social welfare system/youth services system. The voluntary sector.
Key qualities of service systems for drug users Accessibility: How easy/difficult is it to enter the service system?; and are necessary services provided following admission? Coordination: Are services provided in a concerted? Or in haphazard fashion? Do different programs in the system work synergistically? Economy: Are services cost-effective (i.e., given the same total costs, could one achieve better outcomes with a different system?). Coerciveness: What degree of coercion or pressure placed on drug users to seek services? n.b. highest in the criminal justice system but often present in subtle ways (e.g., family pressure) elsewhere. Stigma: Are services viewed as low-status, shameful, and of no value, irrespective of their objective characteristics?
Thank you