Spinal cord injury Miss Fiona Arnold Consultant Neurosurgeon Imperial




40 Slides1.13 MB
Spinal cord injury Miss Fiona Arnold Consultant Neurosurgeon Imperial
Spinal cord injury Injury to the spinal cord /- spinal nerves, leading to complete or partial dysfunction of motor, sensory and autonomic pathways. Main causes: Trauma Degenerative disc disease
Progress 3000 BC, Egyptians: Spinal cord injury is “an ailment not to be treated”. Before 1930: 90% mortality rate Now: nearly normal lifespan due to specialist rehabilitation
Impact on society Trauma Annual incidence 15-40 cases / million Young: 80% age 15-35, 80% male 90% survival Long life span Lifelong sentence of dependence (patient & family) USA 4 billion / year Degenerative disc disease Second highest cause of disability benefit Annual incidence cauda equina syndrome 10-30 cases / million
Traumatic spinal cord injury Mechanisms of injury Neurological presentation Acute management Timing of surgery Future advances - science (fiction)
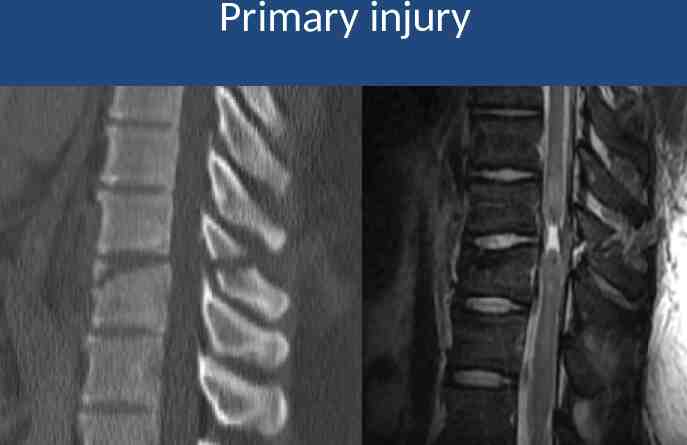
Spinal cord injury Primary injury Due to initial impact Irreversible cell death Functional outcome depends on magnitude & speed of force, and neurological level of injury Secondary injury (?preventable) Initiated by primary injury Ongoing damage over minutes – days Signalling cascade of downstream events Interacting factors: inflammation, oedema, ischaemia, cytotoxicity Autodestruction of neurons, axons &glia
Primary injury from initial impact
One month later
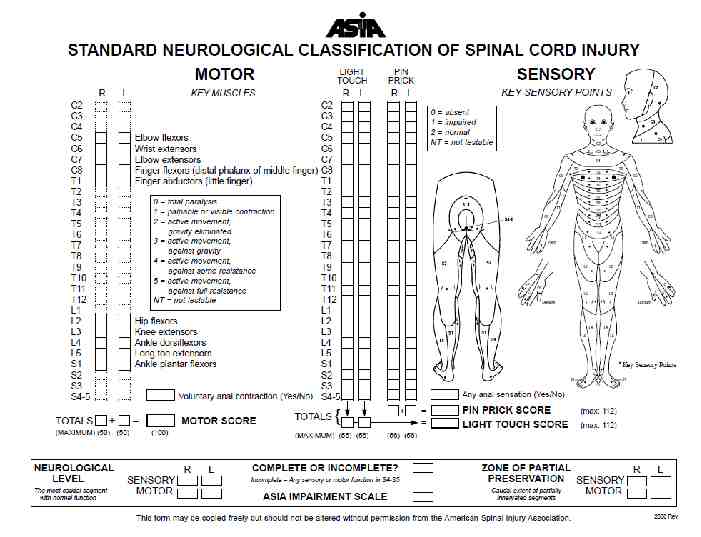
ASIA Neurological Classification of Spinal Cord Injury & Impairment Scale Standardised neurological examination Allow serial observations & comparative studies AMS: Motor (UL, LL, voluntary anal contraction) MRC grade 0-5, 10 key muscles, score 0-100 ASS: Sensory (pin & light) C2-S4/5, score 0-224 NLI : Neurological level of injury AIS: ASIA Impairment Scale
ASIA Impairment Scale A complete no S or M in S4-5 B incomplete S but no M below neuro level (including S4-5) C incomplete M preserved below neuro level ( 1/2 key muscles have grade 3) D incomplete M preserved below neuro level ( 1/2 key muscles have grade 3) E normal intact M & S
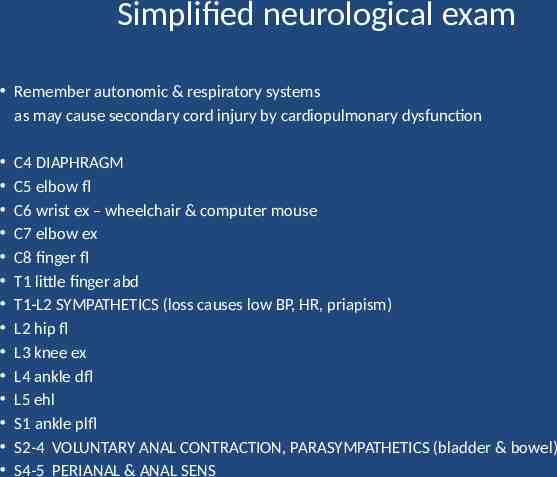
Simplified neurological exam Remember autonomic & respiratory systems as may cause secondary cord injury by cardiopulmonary dysfunction C4 DIAPHRAGM C5 elbow fl C6 wrist ex – wheelchair & computer mouse C7 elbow ex C8 finger fl T1 little finger abd T1-L2 SYMPATHETICS (loss causes low BP, HR, priapism) L2 hip fl L3 knee ex L4 ankle dfl L5 ehl S1 ankle plfl S2-4 VOLUNTARY ANAL CONTRACTION, PARASYMPATHETICS (bladder & bowel) S4-5 PERIANAL & ANAL SENS
Guidelines for Management of Acute Cervical Spine and Spinal Cord Injuries AANS 2001 Evidence selected & evaluated in line with Institute of Medicine Clinical Practice Guidelines 550 page document All “options” (evidence too weak for standards or guidelines), except radiographic evaluation & DVT prophylaxis Due an update Acute Spinal Cord Injury: Reviews J.Neurotrauma (Aug 2011)
Immediate management Resuscitation, spinal immobilisation 30% polytrauma ASIA neuro assess Fine cut CT & reconstructions (BOAST 2, 2008) Reduce secondary injury (“options”): Prevent hypoxia & hypotension (systolic 90) ?MAP 85 ?Methylprednisolone ?Early surgery – compression & instability exacerbate ischaemia
Blood Pressure Avoid hypotension (systolic BP 90 mm Hg) Particular care during anaesthesia HDU monitoring Mean ABP 85 mm Hg for first 7 days to improve spinal cord perfusion Evidence: Laboratory evidence Clinical studies report safe and suggest improved neurological outcome. e.g. Vale et al. (1997) J. Neurosurg.
High Dose Methyprednisolone NASCIS Trials 1990s AANS 2001 “evidence suggesting harmful side effects is more consistent than any suggesting clinical benefit”. Bracken et al. (2012) Cochrane Database Syst. Rev. 8 trials. Improved neurologic outcome if 8hr after injury. Bolus 30mg/kg over 15 min, then 5.4 mg/kg/hr for 23 hr. NASCIS 3: 48hr gives further motor benefit (especially start 3-8hr). No increased complications or mortality. BUT Only 3-5 point AMS increase. See feedback section of Bracken et al.
Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) Fehlings et al. (2012) PLoS ONE OBJECTIVE Evaluate early ( 24 hr) v. late ( 24 hr) decompressive surgery after traumatic cervical spinal cord injury. METHOD Multicentre prospective cohort study in adults, no life threatening injuries, AIS A-D, GCS 13. Outcomes: ordinal change in AIS at 6 months; complication rates & mortality. RESULTS 313 patients (222 follow up). Early, mean 14 5 hr; late, mean 48 29 hr. 19.8% early surgery 2 grade AIS improvement, 8.8% late surgery. Odds of 2 grade AIS 2.8 x higher for early. Equivalent 30-day mortality & complications (24% early & 31% late). CONCLUSION Decompression 24 hr after SCI is safe, and associated with improved neurologic outcome.
STASCIS limitations NOT randomised: time of arrival & “discretion of spinal surgeon”. No mention of injury severity (e.g. ratio of early/late facet dislocations). Facet dislocation – emergent reduction, MRI AFTER (reduction time recorded as surgical time) 1 AIS improvement equivalent for early (37%) / late (41%)
Primary injury
STASCIS, also of interest 40% all AIS A 1 grade improvement; historically 1525% Cervical cohort Rigorous AANS management, inc. induced MAP 85 Pre operative CT & MRI All decompression with instrumented fusion Post operative CT 72hr
Evidence for design of STASCIC Furlan et al. (2009) J. Neurotrauma Animal studies review, favoured surgery 8-24hr Neurological outcome duration of compression LaRosa et al. (2004) Spinal Cord Fehlings et al. (2010) Spine Furlan et al. (2011) J.Neurotrauma Clinical reviews. All level 4 evidence, except one 2b. Early surgery ( 24hr) safe & reasonable option if BP stable.
Urgent surgery Fehlings & Perrin (2006) Spine Urgent reduction of bilateral locked facets with incomplete tetraplegia. Urgent decompression if neurological deterioration.
Subaxial cervical facet dislocation: timing of MRI in relation to reduction MRI: significant disc herniation in 35-50%. Not affect neurological outcome of awake closed reduction. STASCIS: urgent reduction, then MRI Awake closed reduction (cranio-cervical traction) Not if additional rostral injury 65-90% initial success; 30% not maintain reduction Facet fractures may preclude success. 97% arthrodesis in halo. Pre-reduction MRI if: Cannot examine neurologically during closed reduction Open posterior reduction - significant disc is a relative indication for anterior approach
The surgical approach to subaxial cervical spine injuries Dvorak et al. (2007) Spine Literature review and opinion of the Spine Trauma Study Group. 3 categories; includes assessment of discoligamentous integrity and neurological status. Burst, compression & distraction injuries are commonly approached anteriorly. The more severe translation or rotation injuries are commonly approached posteriorly or combined.
Acute management of cervical SCI Conclusions (no level 1 evidence) Avoid hypotension & hypoxia, immobilise spine Fine cut CT MAP 85 (care during anaesthesia) ? Methylprednisolone Urgent surgery if deteriorating neurology or bifacet dislocation with incomplete neurology ? Early decompressive surgery ( 24hr) if no life-threatening polytrauma
Surgical decompression in acute central cord syndrome Lenehan et al., (2010) Spine Literature review & multicentre observational data. Early surgery ( 24hr) had 6.3 point better AMS than late surgery at 12-month (P 0.036), higher chance of improvement in AIS (OR 3.39 at 6-month). It is safe to consider early surgery in patients with AIS C and persistent cord compression. AIS D can be initially observed, with potential later surgery.
Although, Furlan et al. (2011) J.Neurotrauma Literature review & expert opinion “The optimal timing of surgical decompression in central cord injury, or whether surgery is indicated at all, remains unclear.”
Thoracic SCI Thoracic AIS A/B worse outcome than cervical (60% v. 30% 1 AIS) Not significant for incomplete injuries. Thoracic injuries more frequent cardiopulmonary injuries. Cervical segment 9 AMS points. Not the case in thoracic. No equivalent result to STASCIS Furlon et al. (2011) J.Neurotrauma Recommend surgical decompression of the injured spinal cord 24h when medically feasible. Rahimi-Movaghar et al. (2009) Trials Iranian PRCT to compare early ( 24 hr) v. late (24-72 hr) surgery.
Prospective multicentre 2 year follow up of acute traumatic T1-L5 injuries German Association of Trauma Surgery Reinhold et al. (2010) Eur Spine J EPIDEMIOLOGY: 733 operated patients. NEUROLOGY: T-spine injuries worst initial neurology, less recovery, especially AIS A. 61% of AIS A-D improved 1 grade AIS, 73% if AIS C/D, 44% A/B. SURGERY: 52% posterior, 5% anterior, 43% combined. 47% T11-L2 injuries posterior or combined. Surgical approach did not influence neurologic recovery. Posterior patients had better functional & subjective outcome than combined (although posttraumatic radiological deformity was better with combined).
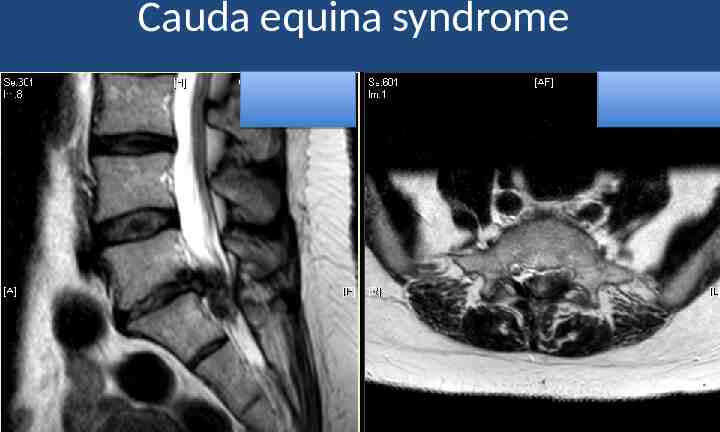
Cauda equina syndrome
Cauda equina syndrome Outcome depends on initial severity & speed of compression, and time to surgery In order of sensitivity to compression: 1) parasympathetics & pudendal nerves (S234) unmyelinated & delicate, central position perianal & genital sens / bladder /sexual / bowel 2) sensory 3) motor Somatic nerve ischaemia irreversible by 4-6hr (e.g. tourniquet)
History Red flags: Sciatica – often bilateral, but can be absent – especially L5/S1 with inferior sequestration Saddle & genital sensory deficit Bladder, bowel & sexual dysfunction Severe low back pain (LBP) Time of onset & speed of progression Time last opened bladder Previous history back pain & sciatica
Exam PIN & LIGHT perianal sensation “Anal wink” & voluntary anal contraction Consider urinary catheter (measure residual) SLR, LL reflexes, power and sensation
Two groups: urinary function & perianal sensation Relevant for timing of surgery & clinical outcome CES-I: incomplete Neurogenic urinary difficulties: loss of desire to void, poor stream, altered sensation, need to strain. Often unilateral or partial saddle & genital sensory deficit. Surgery ideally 12hr Good outcome CES-R: retention Painless urinary retention & overflow incontinence. Usually extensive or complete saddle & genital sensory deficit. Surgery ideally 24hr Poorer prognosis – although 70% socially acceptable long-term outcome.
Cauda equina literature Macfarlane & Greave (1990) B. J Neurosurg CES-I: urgent surgery to prevent progression. CES-R: “The die is cast at the time of the prolapse”. No evidence that emergency surgery influences recovery. Macfarlane & Greave (2002) B. J Neurosurg 70% CES-R good result with surgery at mean of 3.7 days; equivalent 48hr. Recovery of bladder function can continue for years. Surgical exposure should generally be via full laminectomy. Ahn et al. (2000) Spine Significant benefit to surgery 48 hr v. 48hr after CES onset. No difference 24hr v 24-48hr. Kohles et al. (2004) Spine Reassessed Ahn data, found benefit in surgery 24hr. “The earlier the surgery, the better the outcome.”
Conclusion Prompt history, exam and MRI Full explanation and consent procedure Timely and careful surgery Rehabilitation
Future advances - science (fiction) 10% spinal cord axon survival may allow substantial functional recovery (Blight & Hayes) Neuroprotection : prevent secondary injury Avoid hypotension & hypoxaemia, ?steroids, ?early surgery Neuroregeneration (axonal growth / remyelination) : Biological therapies & cell transplantation Retrain sublesional functional networks i.e. central pattern generators “Thought control”: Neuroprosthetic devices
Noninvasive & Directly Applied Biologic Therapies for Neuroregeneration Alter inhibitory environment to allow axonal growth/plasticity . Limitations of animal studies: 90% of studies: treatment applied at time injury. Mainly rodent transection models. No replication studies reproduced the original efficacy. 1 2 3 Clinical trials: Chondroitinase ABC Anti-Nogo antibodies: neutralise myelin inhibition of neurite outgrowth Inhibition of Rho activation: growth cone dynamics & apoptosis
Cellular Transplantation Therapies for Spinal Cord Injury Cell types: schwann, olfactory glial, neural stem/progenitor, bone-marrow stromal Mainly rodent models & rodent cells. Most acute transplantations. Late transplantations rare and poor results.
“Thought control” Neuroprosthetic devices Centre for Neuroengineering, Duke University Wessberg et al. (2000) Nature Neuronal signals from primate motor cortex can control complex movements of a robot arm such as reaching and grasping. O’Doherty et al. (2011) Nature Primate motor cortex controls robotic arm and has artificial tactile feedback through microstimulation of sensory cortex.