Sexual Dysfunction in Male College David Mellinger, MD Students Duke



69 Slides1.24 MB
Sexual Dysfunction in Male College David Mellinger, MD Students Duke University And Steven Kraushaar, PsyD Washington Univ in St. Louis
Objectives Describe the relevant parts of the history and physical examination in a male with sexual dysfunction Compare the available medications used in the treatment of erectile dysfunction in terms of selection Discuss various psychological interventions in treating males with sexual dysfunction
Premature Ejaculation (PE) Ejaculation that occurs sooner than desired Loss of control over ejaculation and Causes distress to either one or both partners
What is too soon? All agree Intravaginal Ejaculatory Latency Time (IELT) of less than 60 seconds is PE Most agree that less than 120 seconds is PE May be dependent on culture and expectation
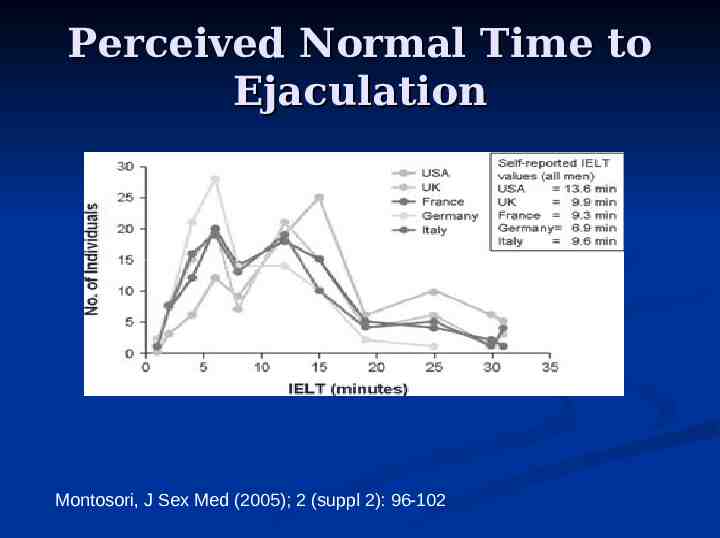
Perceived Normal Time to Ejaculation Montosori, J Sex Med (2005); 2 (suppl 2): 96-102
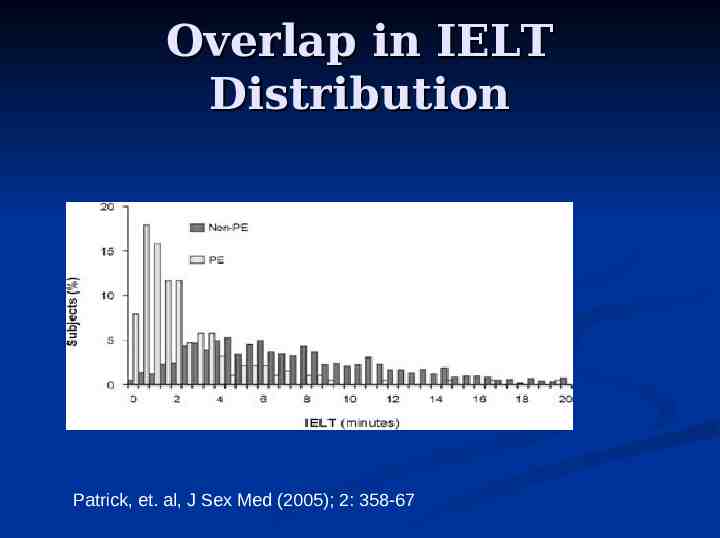
Overlap in IELT Distribution Patrick, et. al, J Sex Med (2005); 2: 358-67
Premature Ejaculation Epidemiology Most common form of sexual dysfunction Prevalence Rates vary from 4-39% ; most general studies in 21-31% range Rates generally not affected by age, marital status, race, or country of residency
Disconnect Between Diagnosed and Reported Prevalence of PE Male patients don’t often “spontaneously” offer up this problem as a complaint Clinicians don’t inquire about this common condition
More on the Disconnect Global Study of Sexual Attitudes and Behaviors 9% of men reported that they had been asked about their sexual health by an MD during a routine visit in the last 3 years 48% of men believe that an MD should routinely ask about sexual health concerns
Why don’t patients report PE Embarrassment Do not “medicalize” the problem Perceive that their provider is not able or willing to address the problem
Why don’t Provider’s Ask about PE Lack of provider comfort in discussing sexuality issues Lack of provider knowledge about PE Low prioritization by medical system of PE No physical comorbidities Time pressure No FDA approved treatment options
What Causes PE Exact etiology not fully known Combination of Physiologic and Psychological Factors Primary PE – “more” neurophysiologic while acquired PE “more” psychological or related to a medical condition
Behavioral Theories of PE Learned Behavior Conditioned from Early Sexual Experiences (Masters and Johnson) Role of Anxiety
PE’s Impact on Men Symonds et. al study* 68% said their confidence generally or in a sexual encounter affected – low “self-esteem” 50% had relationship issues – reluctant to form new relationships or were distressed not satisfying current partner 36% reported being anxious *Symonds et. al., J Sex Mar Ther (2003); 29: 361-370
Important Aspects of History Age at onset of disorder Frequency of PE (Consistent or Intermittent) Circumstance(s) when PE occurs Estimate of Intravaginal Ejaculatory Latency Time (IELT) Any other sexual problems (e.g. ED)? How has it affected your relationship(s)? How has it impacted your sense of wellbeing?
Physical Examination and “Tests” Physical exam is not helpful in diagnosing condition except in some secondary cases where neurologic conditions or prostatitis are entertained No laboratory test available to confirm the diagnosis Can consider psychological tests to assess for anxiety disorder
Treatment for PE Treat underlying cause (e.g. infection) if found Pharmacologic Interventions Behavioral interventions
Pharmacologic Interventions Topical anesthetics Tricyclic antidepressants (TCAs) Selective Serotonin Reuptake Inhibitors (SSRIs) Phosphodiesterase-5 (PDE-5) inhibitors
Topical anesthetics Mode of Action: Desensitize penis and therefore increase IELT Example: Lidocaine/prilocaine cream How to use: Apply to penis 20-30 minutes prior to intercourse, wash off before sex Potential problems Loss of pleasurable sensation for male and partner Contact skin reaction or allergy
TCAs Mode of Action: presumed to act via neurotransmitters involved to inhibit ejaculation Example: Clomipramine How to use: Can take on as needed basis before intercourse or continuous basis Potential problems Side effects Doses and regimens not standardized (Not FDA approved)
Daily vs As Needed Clomipramine In a study* of on demand (OD) clomipramine use in men with PE, 3 factors predicted likely success of OD use Men with IELTs of greater than 60 seconds Men with higher self-reported sexual satisfaction Men who ejaculated 2 or more times per week *Rowland et. al., Int J Imp Res (2004); 16: 354-357
SSRIs Mode of Action: Acts centrally through serotonin receptors in inhibiting ejaculation Example: Paroxetine How to use: Can take OD, on a continuous basis, or a combination of both Potential problems Side effects Doses and regimens not standardized (Not FDA approved)
Oral Therapies* Fluoxetine Paroxetine Sertraline Clomipramine 5- 20 mg/day 10-40 mg/day or 20 mg 3-4 hrs before intercourse (BI) 25-200 mg/day or 50 mg 4-8 hrs BI 25-50 mg/day or 25 mg 4-24 hrs BI *From Amer Urol Assn Guideline, J Urolog (2004); 172: 290-294
PDE-5 Inhibitors Mode of Action: ? having higher cGMP levels might prolong nitrous oxide (NO) effect by delaying ejaculatory emission Prolong erections – may reduce performance anxiety since have improved erections Example: Sildenafil How to use: 25-100 mg 1 hour before sex Potential problems Limited benefit in many studies Side effects Expense
Comparison of Oral Medications Multiple studies proving efficacy in delaying IELT in many SSRIs and TCAs For the SSRIs, paroxetine seems to work the best, with sertraline and fluoxetine close behind Although more efficacious in some studies, almost twice as many adverse effects reported with clomipramine compared with SSRIs The evidence for sildenafil is the weakest, particularly without concurrent erectile dysfunction
Which Option(s) for Patient Consider co-morbidities e.g. atopic dermatitis, anxiety Side effects Expense Ultimately a shared decision between patient and provider
Erectile Dysfunction (ED) “the consistent or recurrent inability of a man to attain and/or maintain an erection sufficient for sexual performance”* *First International Consultation on Erectile Dysfunction, WHO, 1999
Prevalence of ED 5-35% of men have moderate to severe ED Men’s Attitudes to Life Events and Sexuality (MALES) study found prevalence of 16%, 22% in US In the MALES study 8% of men in their 20s reported ED
Epidemiology of ED Age dependent disorder Rate depends on how it is defined Expect the rates will increase as awareness of the condition improves
What causes ED Overall it is a neurovascular phenomenon Sexual stimulation leads to Parasympathetic nervous system enhancement of production of cyclic guanosine monophosphate (cGMP) Smooth muscles relax and blood flows into the penis Filling of the penis, compresses outflow of blood via the veins
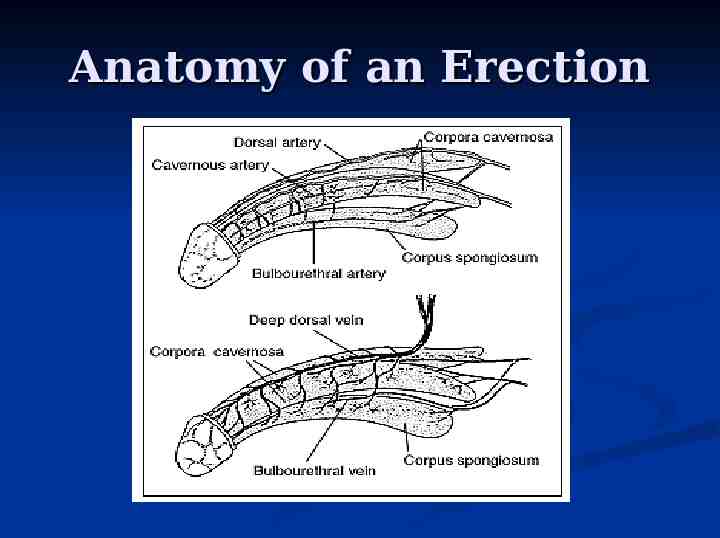
Anatomy of an Erection
Causes of Erectile Dysfunction Physical Causes Vascular (leading cause) Cavernosal Neurologic Hormonal Causes Psychological Factors
Evaluation of Patients with ED Sexual history Onset of Symptoms Duration of Symptoms Circumstances when ED occurs Problems with having an erection Problems with maintaining an erection Libido Concurrent premature ejaculation
Medical History in Patients with ED Any comorbidities? CV disease, Diabetes, Depression, Alcoholism Smoker? Pelvic surgery, radiation, or trauma? Neurologic disease? Other endocrine problems? Recreational or prescribed medication use?
Medications Known to Cause ED Many medications linked to ED Antihypertensives (thiazide diuretics and beta blockers) Antidepressants Hormones
Physical Examination Blood Pressure Measurement Testicular Exam Exam of Penis Vascular and Neurologic Exam if indicated
Laboratory Exam Consider Testosterone if decreased libido Older patients (or others where indicated) do lipid panel and fasted blood glucose Targeted tests in select patients PSA Prolactin
Treatment of ED Identify and Treat Organic Comorbidities and other risk factors Counsel and Educate the Patient and Partner Identify and Treat any Psychosexual Dysfunctions Medications and Devices Surgery
Treatments Lifestyle modifications Weight loss Increase Exercise Smoking Cessation
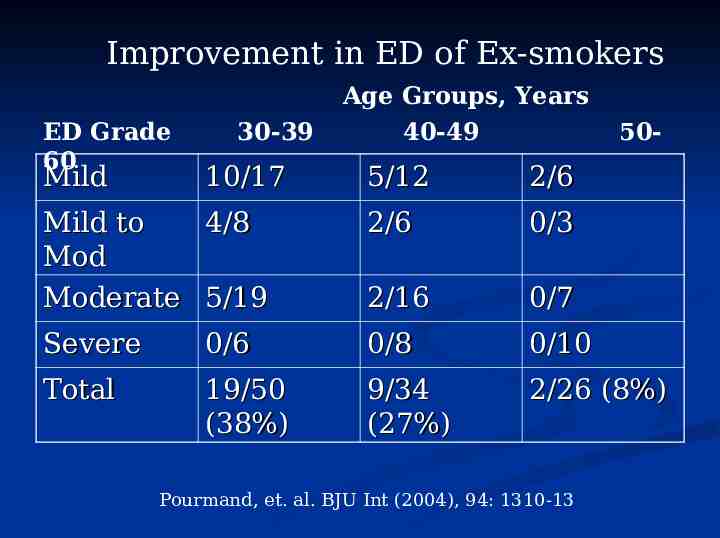
Improvement in ED of Ex-smokers ED Grade 60 Mild 30-39 10/17 Age Groups, Years 40-49 50- 5/12 2/6 Mild to 4/8 Mod Moderate 5/19 2/6 0/3 2/16 0/7 Severe 0/6 0/8 0/10 Total 19/50 (38%) 9/34 (27%) 2/26 (8%) Pourmand, et. al. BJU Int (2004), 94: 1310-13
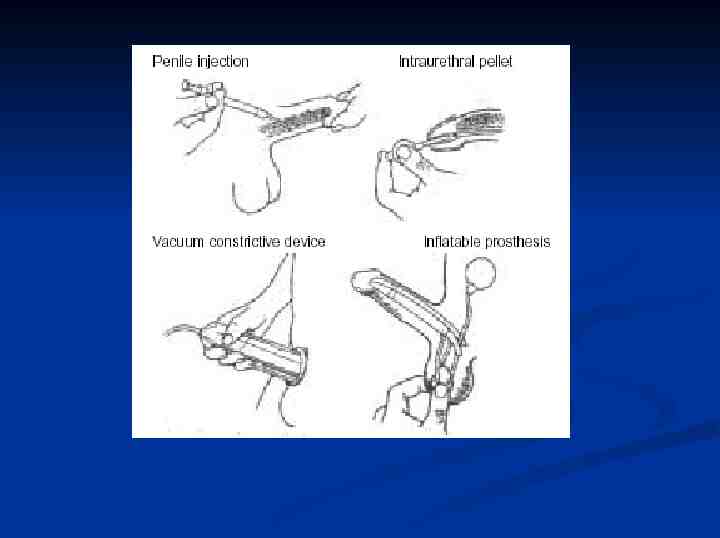
Older Treatments Intracavernosal Injection Vacuum Constriction Devices Intraurethral Alprostadil Suppositories Inflatable Prosthesis Vascular Surgery
Oral Drug Therapies Phosphodiesterase Type 5 (PDE-5) Inhibitors Sildenafil (Viagra) Tadalafil (Cialis) Vardenafil (Levitra) Yohimbe
Use of PDE-5 Inhibitors All three similarly effective 75% of men on medications have satisfactory erection to complete intercourse No large head-to-head trials to compare the 3 available medications Some patients prefer one over the others
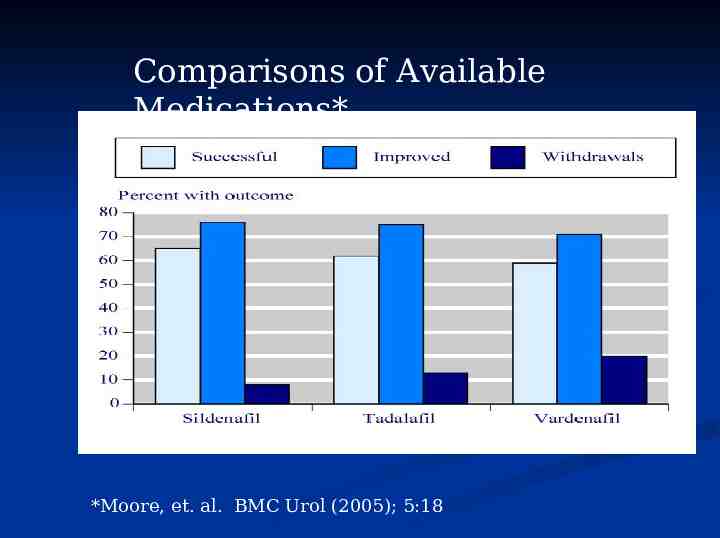
Comparisons of Available Medications* *Moore, et. al. BMC Urol (2005); 5:18
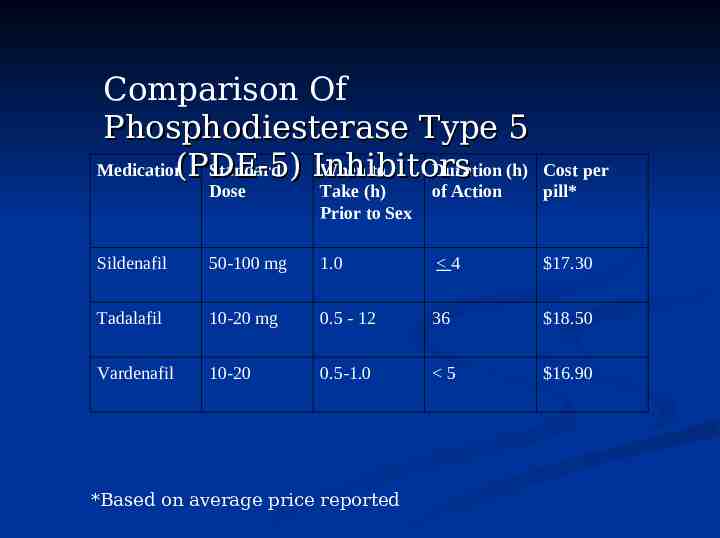
Comparison Of Phosphodiesterase Type 5 Medication(PDE-5) Standard When to Duration (h) Inhibitors Dose Take (h) Prior to Sex of Action Cost per pill* Sildenafil 50-100 mg 1.0 4 17.30 Tadalafil 10-20 mg 0.5 - 12 36 18.50 Vardenafil 10-20 0.5-1.0 5 16.90 *Based on average price reported
What to tell patients about PDE-5 Inhibitors Use Still require sexual stimulation to have erection Sildenafil’s absorption may be reduced by foods – especially fatty foods Expect maximal efficacy in 1 hour (2 hours after tadalafil) First few doses may not be successful – try 6-8 times before giving up
Side Effects Headache Indigestion Flushing Nasal congestion Blue hue to vision
Contraindications Not to use with nitrates (including amyl nitrate) Not to use if severe CV disease Cautious use of vardenafil if has prolonged QT Care if on alpha blocking agents – may cause significant hypotension
Follow-up Recommended for all patients Efficacy Side Effects Any significant change in health status (including new medications)
Why Treatment Failures Food or Drug interactions Timing of Dose ?Maximal Dose Lack of Sexual Stimulation Heavy Alcohol Use Relationship Problems
Yohimbine for ED Derived from the bark of the yohimbine tree in Central Africa Traditionally used to treat all forms of impotence Believed to work through the Central Nervous System An alpha2 adrenoreceptor blocker
Yohimbine for ED Metaanalysis shows yohimbine superior to placebo (Odds ratio of 3.85)* Relatively safe medication Low cost Amer Urol Assn does not recommend its use at this time *Ernst, Pittler; J Urol (1998); 159: 433-436
The Mental Health Perspective 1. 2. Premature Ejaculation Erectile Dysfunction 3. College Health
Sexual History In addition to intake process First awareness of and feelings about anything he considers related to sex Childhood curiosity and exploration Masturbation, including age of first experience, fantasies Student’s socialization based on attitudes and behaviors of family or other significant figures
Sexual History (2) Religious teachings about sexual behavior The Coming Out Process Dating History – “Losing virginity” Relationships vs. “hook-ups” or “fuck buddies” Sexually transmitted infections Sexual experiences initiated by others/abuse When specifically sexual difficulties began
PREMATURE EJACULATION a. b. Conventional Treatments “Stop-and-start” technique Semans (1955) “Squeeze Method” Masters and Johnson (1970)
Limitations Some couples don’t want to interrupt sex after starting. Some students don’t have partners and some partners unwilling to squeeze the penis Techniques viewed as mechanical The focus is on physiological processes and neglect psychological dimensions such as affective communication and sexual pleasure.
Functional-Sexological Treatment First Goal of treatment: Keep the man’s sexual excitement at a level of intensity below that which sets off ejaculation. Achieved by modulating sexual excitement, by monitoring sexual stimulation as well as managing breathing and the muscular tension deriving from sexual activity. (de Carufel, François and Trudel, Gilles (2006) 'Effects of a New FunctionalSexological Treatment for Premature Ejaculation', Journal of Sex & Marital Therapy ,32:2,97 — 114)
Hypothetical Case Example 21 y/o gay Chinese-American (Joe) Referred by medicine due to difficulty maintaining an erection Serious relationship ended 3 months ago, but they still share a suite Low self-confidence, career indecision, interpersonal anxiousness Mood 6/10 Denies SI or HI
ERECTILE DYSFUNCTION Normal to have occasional difficulty achieving an erection Men often feel emasculated and ashamed How could “it” have happened to me? Solitary or infrequently occurring erection difficulty does not mean that a man has a sexual dysfunction. (Morris, 1998)
Erectile Dysfunction (2) Cultural expectations Fears and Myths “Men are taught that their essence is linked to their penis; it is not enough to just have a penis but you must have a big one that stands ready at all times to perform spectacular sexual feats.” (Morris, 1998)
Sensate Focus The cornerstone of sex therapy Helping a couple to focus on sensation rather than performance Structured and flexible Homework Concerns regarding homework discussed in couples session Masters and Johnson (1970, 1986)
College Health Male reluctance to seek help “Sturdy Oak” Manliness Not needing help “The Stud” – “hook-ups” Its just a sprain Brannon (1976)
Men’s health clinic Collaboration, Collaboration, Collaboration Effective referrals Men’s slots
QUESTIONS?