Pharmacy Hot Topics Friday, June 1st 4:45 pm – 5:45 pm Raisa



















































54 Slides2.29 MB
Pharmacy Hot Topics Friday, June 1st 4:45 pm - 5:45 pm Raisa El-Kurdi, PharmD (University of North Carolina) Gregg Wendland, BSPharm (University of Oregon) Jason Goodman, PharmD, MBA (The Ohio State University)
Disclosure No presenter has an actual or potential conflict of interest in relation to this educational activity or presentation.
Finding Your Therapeutic Path to Thrive: ADHD Clinic Raisa El-Kurdi, Pharm.D. PGY1 Community-based Pharmacy Resident UNC Eshelman School of Pharmacy Campus Health Services Chapel Hill NC
Objectives Define the goals of ADHD Clinic as a resource for students. Describe the creation and implementation of ADHD Clinic. Establish the role of a clinical pharmacist in ADHD Clinic. Gain an appreciation for the benefit of inter-professional collaborations between a pharmacist and psychiatrist. Describe the role of team members in ADHD Clinic.
https://pollev.com/multiple choice polls/okVp1dKuD7fAdb2
Brief Review of ADHD ADHD or Attention Deficit Hyperactivity Disorder is a syndrome (not a disease) that is characterized by symptoms of: Inattention Distraction Hyperactivity Impulsivity Affects children, adolescents, and adults
Goals of Treatment Reduce or eliminate symptoms such that patient may engage and be functional in all environments (home, school, work, social). Productivity, Emotional Attention/Focus Impulse control Memory accuracy, & control organization Minimize adverse effects of pharmacotherapy. Closely monitor and provide education.
First Line Therapy Stimulants 70-80% effective Most widely studied Ability to tailor therapy Significant patient to patient variability 2 Classes of Stimulant Medication Methylphenidate: DA Amphetamine: NE/DA
CNS Stimulant Black Box Warnings Abuse Potential CNS stimulants, including methylphenidate-containing products and amphetamines, have a high potential for abuse and dependence. Administration for prolonged periods of time may lead to drug dependence. Assess the risk of abuse prior to prescribing and monitor for signs of abuse and dependence while on therapy Cardiovascular Events Misuse of amphetamines may cause sudden death and serious cardiovascular adverse events Sudden death in patients who have heart problems or heart defects Stroke and heart attack in adults Increased BP and HR
Considerations for Selecting Stimulant All stimulants are equally efficacious regardless of age, gender, and formulation. Interpatient variability Assessment/HPI Including treatment history (treatment naïve?) History of substance abuse? Lifestyle/Class schedule Severity of condition Start with ER or IR? Conflicting data in literature Consider how quickly you can follow-up Pill burden and multiple dosing Patient’s goals (schedule, domains, resources) Cost Brand vs. Generic
Managing Stimulant Side Effects Adverse Effect Anorexia GI Upset Insomnia Irritability Dysphoria “Zombie” State Increased BP/HR Tics Hallucinations Management High-calorie meal when stimulant effect is low. Consider cyproheptadine at bedtime Give with or after food; consider lower dose Take as early as possible; discontinue afternoon dose; consider sedating drug at bedtime Evaluate for comorbid conditions; reduce dose or increase dose Reduce dose; consider alternative stimulant Reduce dose; consider alternative stimulant Monitor; reduce dose or switch agents Reduce dose, consider alternative stimulant Discontinue stimulant
What is ADHD Clinic?
Mission The clinic's mission is to practice as a multi-disciplinary health care team, in order to develop a specialized approach to achieve a therapeutic path for students to thrive with ADHD.
Implementation Process
Environmental Scan CADDRA 4th ed. 2018
Environmental Scan-Organization Policies Liability Sustainability Revenue Generator
Interdisciplinary Team Model Campus Health -Psychiatrist -Pharmacist -Administrative Assistant The Learning Center - Academic coach -Peer Tutors Accessibility Services -Accessibility/Testing Coordinators Community Resources - Cognitive Behavioral Therapist - ADHD coach - Therapist
Workflow
Sessions 30 minutes in length 20 minute allotment with pharmacist Vitals Q/A Dose adjustments 10 minute allotment with the psychiatrist Reviews completed encounter note Validates prescriptions Further evaluation for complex patients
Monitoring Therapy Every 3 months (4 months during the summer months) – mandatory for refills Vitals and Notes Blood pressure/Heart rate Side effects Response to therapy Compliance Co-morbidities Tobacco, alcohol and or drug use Patient goals and resources
Benefits Students Personalized patient centered care Assess regimen appropriateness Patient education and alternative resources Develop strategies Patient comorbidities assessed Organization Medication education, management, reconciliation and monitoring with the aid of a pharmacist Allows for a more efficient and effective workflow Increase in new patient appointment availability Allows for closer patient monitoring and adherence to organizational stimulant policy Increase in revenue Establish provider patient relationships.
References Ustun B, Adler LA, Rudin C, et al. The World Health Organization Adult Attention-Deficit/Hyperactivity Disorder Self-Report Screening Scale for DSM-5. JAMA Psychiatry. 2017;74(5):520–526. doi:10.1001/jamapsychiatry.2017.0298 Biol Psychiatry 2011;69:e145– e157 doi:10.1016/j.biopsych.2011.02.036 2011 Society of Biological Psychiatry Pliszka SR. The neuropsychopharmacology of attention-deficit/hyperactivity disorder [review]. Biol Psychiatry. 2005;57:1385-1390. Long-term efficacy and safety of treatment with stimulants and atomoxetine in adult ADHD: A review of controlled and naturalistic studies. Fredriksen, Mats et al. European Neuropsychopharmacology , Volume 23 , Issue 6 , 508 - 527 Adult Attention Deficit-Hyperactivity Disorder. Volkow, N.D. Swanson, J.M n engl j med 369;20 nejm.org November 14, 2013 Dopheide and Pliszka. PHARMACOTHERAPY Volume 29, Number 6, 2009. Attention-Deficit–Hyperactivity Disorder: An Update Maintenance and Follow-up Care for Adults with ADHD: A Guide for Primary Care Providers by Anthony L Rostain, MD, MA Craig B.H. Surman Editor ADHD in Adults. A Practical Guide to Evaluation and Management. Curr Psychiatry Rep. 2014 Mar; 16(3): 436. Zulauf, C, Sprich, S, Safren S, et al. The Complicated Relationship Between Attention Deficit/Hyperactivity Disorder and Substance Use Disorders. Surman, C.B., ADHD in Adults – A practical guide to Evaluation and Management. 2013
Questions PGY1 Community Pharmacy Resident UNC Eshelman School of Pharmacy Campus Health Services, Chapel Hill, NC Email: [email protected]
PHARMACY CLINICAL SERVICES: CONTRACEPTIVE AND NALOXONE PRESCRIBING GREGG WENDLAND, RPH PHARMACY MANAGER UNIVERSITY OF OREGON HEALTH CENTER
PHARMACIST CLINICAL/COGNITIVE SERVICES ‘They’re not going to pay you 27 per hour to just count and pour and lick and stick’ – Dr. Lee Strandberg, Pharmacy Socioeconomics, Oregon State University College of Pharmacy, circa 1993.
PHARMACIST CLINICAL SERVICES DEFINED For the purposes of this presentation, we will focus discussion on services outside the traditional prescription processing area and that do not require a CDTM agreement. An early and prevalent example is vaccine delivery. Oregon currently also allows pharmacists to prescribe contraceptives (pills, patch, ring, injection) as well as naloxone under a set of defined protocols.
CONSIDERATIONS Is your pharmacy a department of the Health Center or associated with a different campus unit (e.g. College of Pharmacy)? Is the service duplicative of one offered by other providers in the clinic? (Contraceptives yes, naloxone no) If yes, is the service a bandwidth expansion or competition? Is the service accessible, valuable, and sustainable (cost effective)?
NALOXONE PRESCRIBING OAR 855-019-0460Naloxone - Delivery of Care (1) A pharmacist can prescribe naloxone and the necessary medical supplies for opiate overdose training. (2) A pharmacist can prescribe naloxone and the necessary medical supplies to an individual or entity seeking naloxone. (3) The pharmacist shall determine that the individual (or the individual on behalf of an entity) seeking naloxone demonstrates understanding of educational materials related to opioid overdose prevention, recognition, response, and the administration of naloxone. (4) The pharmacist may prescribe naloxone in any FDA approved dosage form and the necessary medical supplies needed to administer naloxone. (5) The pharmacist shall dispense the naloxone product in a properly labeled container. (6) Naloxone may not be prescribed without offering to provide oral counseling to the authorized recipient, which may include dose, effectiveness, adverse effects, storage conditions, and safety. (7) The pharmacist must document the encounter and the prescription, and maintain records for three years. (8) Any person, having once lawfully obtained naloxone may possess, distribute or administer it for the purpose of reversing opiate overdose.
PHARMACIST TRAINING Oregon State University has published a training module to prepare pharmacists for this service. https://pace.oregonstate.edu/catalog/naloxone-opioid-overdose-prevention-recognition-response National (ACPE-approved) training may be found at https://www.pharmacytimes.org/landing/787 (free, expires September 2018). Additional ACPE-approved CE with focus on legal aspects and 'Good Samaritan laws: https://www.uspharmacist.com/ce/expanding-access-to-naloxone-role (free, expires October 2018)
RESOURCES Prescribe to Prevent: http://prescribetoprevent.org/pharmacists/pharmacy-basics/ Oregon Health Authority: http://www.oregon.gov/oha/PH/PREVENTIONWELLNESS/SUBSTANCEUSE/OPIOIDS/Pages/naloxone.asp x#pharmtoolkit (includes interactive map)
TARGET GROUPS Campus Police Department/Campus Safety Resident Advisors for campus Residence Halls Greek Life Organizations University Substance Abuse Prevention office Other first responders Interested individuals
DOSAGE FORMS There are many forms available. Members of buying groups (like MMCAP) may get special pricing on select products. Some manufacturers may offer a limited number of free doses to Universities.
THE UO EXPERIENCE SO FAR First outreach: training the UO campus Police Department on the proper use of Naloxone (December 2017) and assisted with sourcing product for the department. Ongoing promotion at the pharmacy and collaboration with campus partners and student groups.
CONTRACEPTIVE PRESCRIBING 855-019-0415Contraceptive - Training Program (1) Only a pharmacist, who has completed a Board approved Accreditation Council for Pharmacy Education (ACPE) accredited educational training program related to the prescribing of contraceptives by a pharmacist, may prescribe injectable hormonal contraceptives and self-administered hormonal contraceptives for a patient. (2) A pharmacist must submit a copy of the certificate of completion of training to the Board within 15 days of completion. (3) A pharmacist must maintain the certificate of completion and make available upon request.
INTAKE PROCESS: US MEC-BASED SELF-SCREENING QUESTIONNAIRE (WE ALSO RECOMMEND USING A SHORTER PREQUALIFICATION FORM TO SCREEN FOR 'DEAL-BREAKERS' LIKE MIGRAINE WITH AURA)
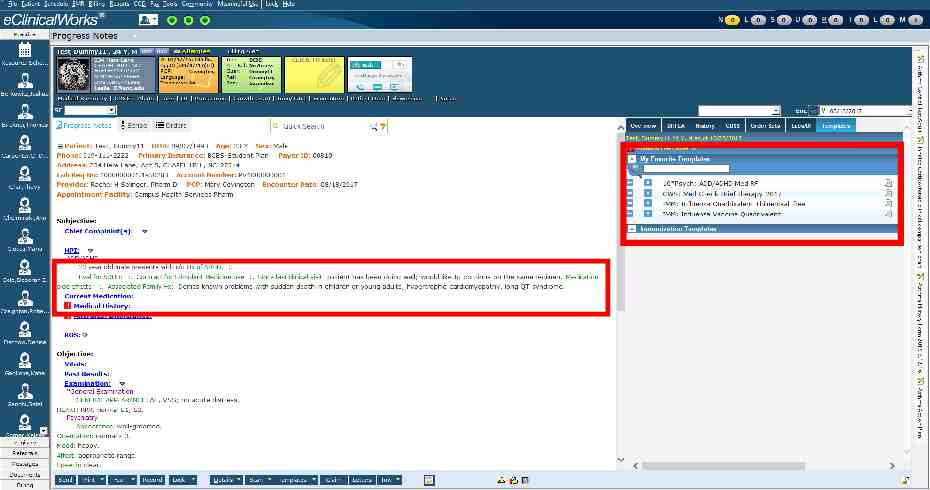
INTERFACING WITH THE CLINIC Even though the pharmacy is technically providing this service autonomously (without a CDTM in place), we still consider ourselves part of the UHC care team. For this reason, the self-screening questionnaire was converted to a template in Medicat, the clinic's Electronic Health Record. Prescribing pharmacists also enter prescribed medications into RCopia, Medicat's prescribing module. Added a question to the self-screening questionnaire to confirm that the patient was not denied a prescription/refills for contraceptives by a UHC clinician.
LESSONS LEARNED: POSITIVES Students appreciate the enhanced access to contraceptive prescriptions. The program frees up appointment slots for other clinicians to handle additional non-routine or complex cases. More than 100 unique patients seen since March 2017. The program has yielded over 250 additional prescriptions and more than 7000 in additional revenue in this time.
LESSONS LEARNED: OPPORTUNITIES TO IMPROVE The structure of the program which doesn't allow pharmacy to require appointments presents challenges when short-staffed or there is high demand. This can lead to patient disappointment when they are unable to have a consultation 'on-demand'. The program is configured with the theory that a consultation session will take approximately 15 minutes. Since pharmacists have to do all of their own charting and data entry, it often takes longer than this. Clinic billing practices limit the ability to charge the 'going rate' for a consult ( 15 vs. 50-60 in the community). Government-funded programs (e.g. CCARE) only recently began paying for pharmacist-prescribed contraceptives and still will not cover the consultation fee.
QUESTIONS? Feel free to email me at [email protected] with any follow up questions.
Jason Goodman, PharmD, MBA Office of Student Life Student Health Services
Office of Student Life Student Health Services Objective Discuss up and coming pharmacist services and issues impacting student health center pharmacies. 46
Office of Student Life Student Health Services Cholera Vaccine Misconceptions/Misuse of stimulants Supplements to NCAA athletes 47
Office of Student Life Student Health Services Cholera Vaccine Acute, diarrheal illness Infection of the intestine with the toxigenic bacterium Vibrio cholerae serogroup O1 or O139 2.9 million cases and 95,000 deaths occur each year around the world Mild or without symptoms, but can sometimes be severe 10% of those infected will have severe disease Death can occur within hours https://www.cdc.gov/cholera/general/index.html 48
Office of Student Life Student Health Services Cholera Vaccine Administered at least 10 days prior to exposure No food or drink 60 minutes before or 60 minutes after administration 1 buffer packet 1 active packet 1 dose Reconstituted in purified bottled or spring bottled water Must be reconstituted within 15 minutes of removal from freezer Must be administered within 15 minutes of reconstitution Stored in freezer (–13 F to 5 F) Patient Monitoring 49
Office of Student Life Student Health Services Cholera Vaccine Cost Administration Fee Billing?!?! 50
Office of Student Life Student Health Services Abuse/misuse of stimulants Netflix Original “Take your pills” Arria A et.al. (2017), “Do college students improve their grades by using prescription stimulants nonmedically?”, Addictive Behaviors, 65: 245–249. Arria A et.al. (2017), “Perceived academic benefit is associated with nonmedical prescription stimulant misuse among college students.” Addictive Behaviors, 76: 27–33. 51
Office of Student Life Student Health Services Guidance/advice/supplying supplements to NCAA athletes NCAA Sport Science Institute Performance enhancing drugs Dietary Supplements https://dfsaxis.com/users/login Alcohol and other recreational drug prevention Drug Testing Program 52
Office of Student Life Student Health Services Guidance/advice/supplying supplements to NCAA athletes (Continued) NSF Certified for Sport http://www.nsfsport.com/certified-products/ App Smart Search Capabilities and Barcode (UPC) Scanning Search by supplement type or by goal Side-by-side comparison features allow you to make smart and effective decisions about which supplements best fit your fitness needs. Favorites and Push Notifications for New Certified Products 53
Office of Student Life Student Health Services The Cholera Vaccine is live and administered orally True False Questions 54