Maximize Your Billings in Hospice and Palliative Care


66 Slides492.78 KB
Maximize Your Billings in Hospice and Palliative Care
Disclaimer The information contained in this presentation is thought to be as accurate and up-to-date as possible as of the time the slides were created CMS and other payors may change their policies, and their interpretation, frequently and unpredictably Ultimate responsibility for decisions on coding and billing for services lies with the provider Check with your Medicare Administrator Contractor for specific questions; especially with the new codes Reimbursement based on 2019 NC rates
Learning Objectives Discuss the elements required to meet certain Evaluation/Management Codes Understand Advance Care Planning Codes Discuss new codes for 2017-2019 and changes to existing codes Develop a sense of billings/month/year Develop a quality improvement plan to develop processes for implementation
Palliative Care Provider Billing All billings Medicare Part B Billings paid based on physician fee schedule – Medicare pays 80% of allowable Must show additional 20% billed to patient or insurance/Medicaid NP/PA receive 85% of physician rate Can bill as attending or consulting Paid by the MACs (Medicare Administrator Contractor)
Coding is determined by o Who are you? o Who is the patient? o Where is the patient? o Time or complexity? o Nuances to our field
General Guidelines o Proper Documentation Includes Care Setting Reason for Visit Relevant history, physical, diagnostic labs Clinical diagnosis and assessment Plan of care Date and legible identity of provider
Evaluation and Management (E/M) Codes o Determined by: Patient type Patient care setting Level of E/M service billed
Patient Care Setting/Type o Inpatient Skilled Nursing Home/ Hospital/GIP Hospice: Initial vs. Subsequent o Outpatient ALF/Domiciliary/Home/Routine care Hospice: New vs. Established
Patient Type o New – patient has not been seen by the physician or the physicians in the same sub specialty group within the past 3 years. o Established – patient has received face to face service from the physician or member of the same sub specialty group within 3 years. Example: Patient discharged from PC seen 2 years later in the clinic setting – established patient
Consulting Codes o No longer recognized by CMS o Can use with insurers so need to understand when to use o Usually pay at higher rate o 99241-99245 o 99251-99255
Types of Coding o There are two methods for determining CPT Levels Intensity (Component or Element coding) Time Intensity trumps time!
Intensity o If you complete a complex visit and fulfill/exceed all the key components in less than the typical time – you still bill at the higher code. o Example - Subsequent hospital care 99232 typically 25 minutes 99233 typically 35 minutes I meet the key components for a 99233 in 20 minutes so I bill the 99233.
Intensity vs Time o How should you bill? General rule of thumb 75-85% intensity, 15-25% time May somewhat depend on practice setting and # of family meetings conducted
Intensity vs Time o Need to understand both well o Common mistake is to just bill on time o When 50% time is spent in coordination and counseling, time code should be used. (face to face time in outpatient setting/face to face floor time in inpatient unit)
Evaluation & Management Codes First, determine which CPT E&M code to use Location of the patient New vs. Established (outpatient) Initial vs. Subsequent (inpatient) Then choose right “level” of service Most often at levels 3, 4 or 5 in our world Based on documentation of Key Components: 1. History 2. Exam, and 3. Medical decision making OR Time counseling/coordination of care
Billing by Intensity Key elements in selection of level o History Problem focused Expanded problem focused Detailed Comprehensive o Physical – same as above o Medical decision making Straightforward, Low, Moderate, High
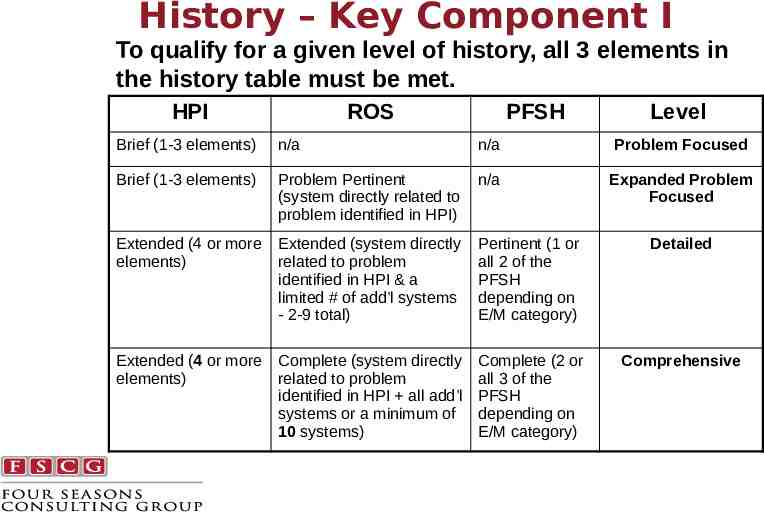
History – Key Component I To qualify for a given level of history, all 3 elements in the history table must be met. HPI ROS PFSH Level Brief (1-3 elements) n/a n/a Problem Focused Brief (1-3 elements) Problem Pertinent (system directly related to problem identified in HPI) n/a Expanded Problem Focused Extended (4 or more elements) Extended (system directly related to problem identified in HPI & a limited # of add’l systems - 2-9 total) Pertinent (1 or all 2 of the PFSH depending on E/M category) Detailed Extended (4 or more elements) Complete (system directly related to problem identified in HPI all add’l systems or a minimum of 10 systems) Complete (2 or all 3 of the PFSH depending on E/M category) Comprehensive
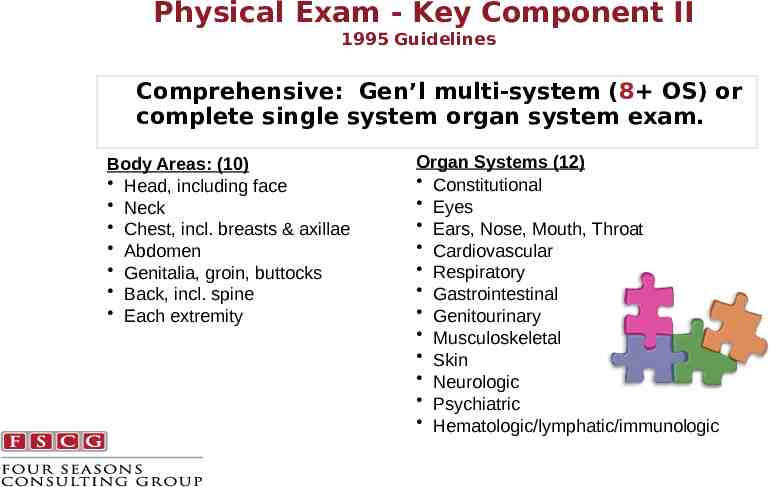
Physical Exam - Key Component II 1995 Guidelines Comprehensive: Gen’l multi-system (8 OS) or complete single system organ system exam. Body Areas: (10) Head, including face Neck Chest, incl. breasts & axillae Abdomen Genitalia, groin, buttocks Back, incl. spine Each extremity Organ Systems (12) Constitutional Eyes Ears, Nose, Mouth, Throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Skin Neurologic Psychiatric Hematologic/lymphatic/immunologic
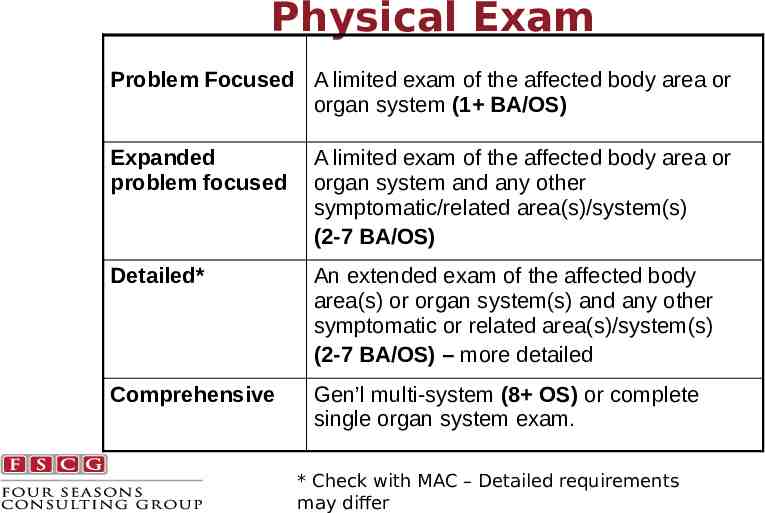
Physical Exam Problem Focused A limited exam of the affected body area or organ system (1 BA/OS) Expanded problem focused A limited exam of the affected body area or organ system and any other symptomatic/related area(s)/system(s) (2-7 BA/OS) Detailed* An extended exam of the affected body area(s) or organ system(s) and any other symptomatic or related area(s)/system(s) (2-7 BA/OS) – more detailed Comprehensive Gen’l multi-system (8 OS) or complete single organ system exam. * Check with MAC – Detailed requirements may differ
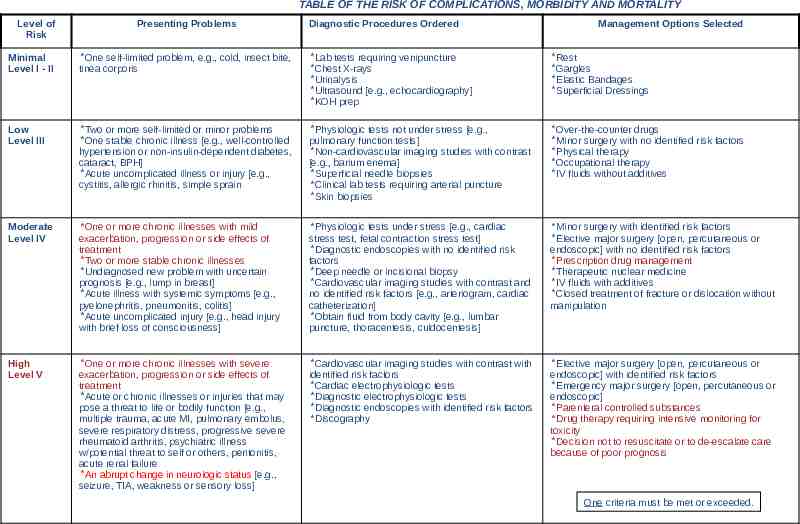
Complexity of Medical Decision Making – Key Component III Complexity of Medical DecisionMaking: Data ordered or reviewed Diagnosis and Management Risk of significant complications, morbidity and mortality
TABLE OF THE RISK OF COMPLICATIONS, MORBIDITY AND MORTALITY Level of Risk Presenting Problems Diagnostic Procedures Ordered Management Options Selected Minimal Level I - II *One self-limited problem, e.g., cold, insect bite, tinea corporis *Lab tests requiring venipuncture *Chest X-rays *Urinalysis *Ultrasound [e.g., echocardiography] *KOH prep *Rest *Gargles *Elastic Bandages *Superficial Dressings Low Level III *Two or more self-limited or minor problems *One stable chronic illness [e.g., well-controlled hypertension or non-insulin-dependent diabetes, cataract, BPH] *Acute uncomplicated illness or injury [e.g., cystitis, allergic rhinitis, simple sprain *Physiologic tests not under stress [e.g., pulmonary function tests] *Non-cardiovascular imaging studies with contrast [e.g., barium enema] *Superficial needle biopsies *Clinical lab tests requiring arterial puncture *Skin biopsies *Over-the-counter drugs *Minor surgery with no identified risk factors *Physical therapy *Occupational therapy *IV fluids without additives Moderate Level IV *One or more chronic illnesses with mild exacerbation, progression or side effects of treatment *Two or more stable chronic illnesses *Undiagnosed new problem with uncertain prognosis [e.g., lump in breast] *Acute illness with systemic symptoms [e.g., pyelonephritis, pneumonitis, colitis] *Acute uncomplicated injury [e.g., head injury with brief loss of consciousness] *Physiologic tests under stress [e.g., cardiac stress test, fetal contraction stress test] *Diagnostic endoscopies with no identified risk factors *Deep needle or incisional biopsy *Cardiovascular imaging studies with contrast and no identified risk factors [e.g., arteriogram, cardiac catheterization] *Obtain fluid from body cavity [e.g., lumbar puncture, thoracentesis, culdocentesis] *Minor surgery with identified risk factors *Elective major surgery [open, percutaneous or endoscopic] with no identified risk factors *Prescription drug management *Therapeutic nuclear medicine *IV fluids with additives *Closed treatment of fracture or dislocation without manipulation High Level V *One or more chronic illnesses with severe exacerbation, progression or side effects of treatment *Acute or chronic illnesses or injuries that may pose a threat to life or bodily function [e.g., multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness w/potential threat to self or others, peritonitis, acute renal failure *An abrupt change in neurologic status [e.g., seizure, TIA, weakness or sensory loss] *Cardiovascular imaging studies with contrast with identified risk factors *Cardiac electrophysiologic tests *Diagnostic electrophysiologic tests *Diagnostic endoscopies with identified risk factors *Discography *Elective major surgery [open, percutaneous or endoscopic] with identified risk factors *Emergency major surgery [open, percutaneous or endoscopic] *Parenteral controlled substances *Drug therapy requiring intensive monitoring for toxicity *Decision not to resuscitate or to de-escalate care because of poor prognosis One criteria must be met or exceeded.
Coding Using Components History Examination Complexity of Medical Decision-Making the E&M Level
Coding Pearls o All subsequent and established visits except office/clinic visits History, physical & medical decision making - only need 2 out of 3 key components to bill for a particular level of care HPI – all subsequent visits only need interval history (no need for PMH, SH, FH) The most important component is medical complexity – assessment and plan, so have thorough documentation in this section
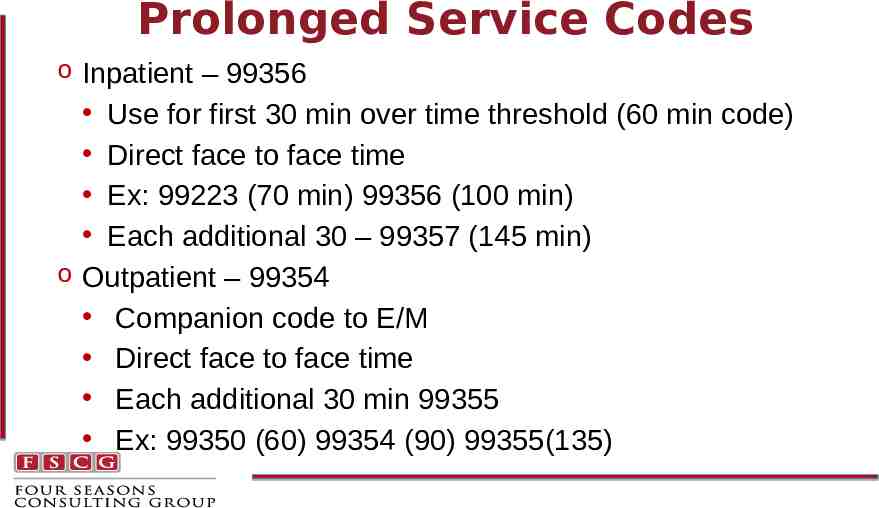
Prolonged Service Codes o Inpatient – 99356 Use for first 30 min over time threshold (60 min code) Direct face to face time Ex: 99223 (70 min) 99356 (100 min) Each additional 30 – 99357 (145 min) o Outpatient – 99354 Companion code to E/M Direct face to face time Each additional 30 min 99355 Ex: 99350 (60) 99354 (90) 99355(135)
Prolonged Service Codes o Used when a physician provides prolonged service involving direct patient contact that is beyond the usual service (typical time) in either the inpatient or outpatient setting CPT book Direct – includes F2F and Floor time in the hospital and just F2F time in the outpatient setting (including NH), however Medicare requires inpatient F2F o The prolonged time does not have to be continuous but in- out times must be recorded o Each code is reported separately in addition to appropriate E/M service code o 99356, 99354 – 60 min beyond usual time – 30 min threshold o 99357, 99355- 30 min beyond initial code – 15 min threshold
Prolonged Service Codes o Documentation should include: Start and end time of the visit Date of visit Duration of visit Content of visit Documentation to support rendering provider furnished direct F2F time
2017 - Non F2F Prolonged Service Codes o 99358 – prolonged E/M service before and/or after direct patient care – first hour* o 99359 – prolonged E/M services before and/or after direct patient care – each add 30 min o Palliative Care Only!! (not Part A) “These codes would provide a means to recognize the additional resource costs of physicians and other billing practitioners, when they spend an extraordinary amount of time outside of an E/M visit performing work that is related to that visit and does not involve direct patient contact (such as extensive medical record review, review of diagnostic test results or other ongoing care management work.”) * 31 minutes you can bill 99358, 76 min for both codes
New Non F2F Prolonged Service Codes o Must be directly related to a specific F2F visit that was o o o o provided on same or different day Time must be performed by the billing provider Time thresholds much be documented Mid-point needs to be passed to bill Cannot be billed during complex CCM or TCM codes
Reimbursement 99358 – 109.71 99359 - 52.76
Scenario 1 68 yo WM hospitalized for exacerbation of COPD with underlying pneumonia. A comprehensive history & physical, with high MDM is performed and 20 minutes is spent discussing goals and treatment options, hence an ACP code is submitted. Later in the day, the physician spends 35 minutes reviewing the diagnostic tests and, discusses the case with the hospitalist and intensivist. What is the correct CPT codes for both of these visits which occurred on the same day?
Scenario 1 99358 – non F2F prolonged visit code 99223 – comprehensive H&P, High MDM 99497 – ACP Reimbursement Day 1 110 200 75 385
Scenario 2 83 yo WF with metastatic colon cancer and mild dementia who is being transferred from the SNF back to the home setting. Palliative Care PA performs established visit with comprehensive history, PE and complex MDM. After seeing the patient, the PA calls the PCP with an update and medication change, followed by discussion with the SW on resource needs in the home. Called daughter and spoke for 35 min. He spends a total of 76 min on these calls and care coordination. o What is the correct CPT codes for these visits?
Scenario 2 o 99350 - established home visit o 99358 – non F2F prolonged service code o 99359 – add on to above for non F2F time Reimbursement o Code 175 110 53 350 o 350*.85 287 (PA rate)
Extending a E/M code that is based on components/intensity is different than “time based coding”
Quiz Time Subsequent visit codes 99231 – 15 min 99232 – 25 min 99233 – 35 min o Subsequent hospital visit for lung cancer patient with nausea. You spent 10 min reviewing notes, 15 min obtaining detailed GI history, and 5 min with exam. You diagnose gastroparesis and spend 25 minutes discussing etiology/ treatment. How should you bill? Total time 55 min A. Time based billing – 99233 99356 B. Complexity based with extender 99232 99356 C. Complexity visit 99232
Quiz Time o Base Code – 99232 Based on expanded problem o o o o focus history and exam with moderate complexity of medical decision making; Billed by intensity Counseling around treatment – 25 minutes; does not meet the 50% requirement Typical time for 99232 is 25 minutes Time over base code 55 min - 25 min 30 Bill extender code since 30 min over threshold (25 30) 99356
Distinguish Elements for Time Based Billing
The 50% Rule o When these medically necessary activities and/or coordination of care constitute more than 50% of the physician/ patient and/or family encounter (face-to-face time in the office or other outpatient setting or floor/unit time in the hospital or nursing facility) time may be considered the key or controlling factor to qualify for a particular level of E/M service. This includes time spent with those individuals who have assumed responsibility for the care of the patient or decision making, regardless of whether they are family members (e.g., child’s parents, foster parents, person acting in locum parentis, legal guardian). AMA Principles of CPT coding, Rev Edition; 2010
Time-Based Coding - Outpatient Face to Face Time for office and other outpatient settings – face-to-face time is defined as only that time which the physician spends face to face with the patient and/or family. Therefore, Non face-to-face time (pre- and post-encounter time) is NOT included in the time component for outpatient work (assumed to be included in the CPT level).
Billing by Time Document rationale for using time Diagnostic results, impressions, and/or recommended diagnostic studies Prognosis Risks and benefits of management or treatment choices Instructions for management (treatment and/or follow-up) Importance of compliance with chosen management (treatment) options Treatments initiated or adjusted Risk factor reduction Patient and family education Must document the actual time (minutes) and include the notation, “more than 50% of the time was spent in counseling and coordination of care for .” 40
Questions? Billing by intensity or time? Prolonged service codes Non F2F prolonged service codes
Understanding Advance Care Planning Codes and When to Use
Rationale Only 4 in 10 Americans 65 years old have advance directives 89% patients feel doctors should discuss Advance Care Planning, however for those 65 years old only 17% state they have had a conversation with their physician 90% Americans prefer to die at home, yet only a third of all deaths occur in this setting 25% total Medicare spending occurs in the last year of life 10 FAQ’s: Medicare’s Role in End-of-Life, Nov 2015, Kaiser Foundation Fact Sheet
What Constitutes Advance Care Planning? Understanding health care options that are available for end-of-life care Deciding what treatments align with patient’s goals Sharing personal values and goals of care May include filling out/discussion of advance directives written instructions to help guide care, include living wills, health care power of attorney, and many of the state directives documents No limit of number of Advance Care Planning codes/beneficiary
Who Qualifies for Advance Care Planning Services? o Individuals with end-stage chronic illnesses o Individuals facing emergent and high-risk surgeries, or who experience sudden event o Individuals with dementia or mental illnesses o Individuals who lack decision making capacity o Advance Care Planning codes may be used with a wellness visit
Who is Qualified to Bill? o Physician or Non-Physician Practitioner (QHP)* 1. Incident to Rules requirements met 2. Must be Qualified Clinical staff 3. Under Direct supervision of Physician or Non-Physician Practitioner Social Worker, Registered Nurse, Chaplain Other clinical staff – Psychologists, Case Managers Billed under provider’s National Provider Identifier (NPI) number *QHP (Qualified Health Professional) applicable state law and scope of practice requirements must be met
“Incident to” Requirements o Physician or Non-Physician Practitioner performs initial service o Provider directly supervises and must be present o Manage, participate and meaningful contribution by provider o Incident to applies to office/clinic setting and rural home setting where no home health agency is available o Not hospital/nursing home setting
Documentation Required CMS did not specify “standards or requirements” for billing codes, however must demonstrate – Who is the supervising physician – With whom the conversation occurred – Where the service is provided – Contents of the conversation that occurred – Patient/surrogate acknowledges Advance Care Planning service – Number of minutes spent (Time Based Codes)
Frequently Asked Questions Does the patient need to be present? No, can be with surrogate Can you provide telephonically? No, requires face-to-face visit Can more than one provider bill? Yes Is there a limit to the physician specialty? No Is there a limit to the number of codes billed? No Can Advance Care Planning codes be billed at same time of Transitional Care Health Management and Chronic Care Management codes? Yes Can Advance Care Planning codes be be billed together with routine office visit, hospital visit and nursing home visit E/M charges? Yes
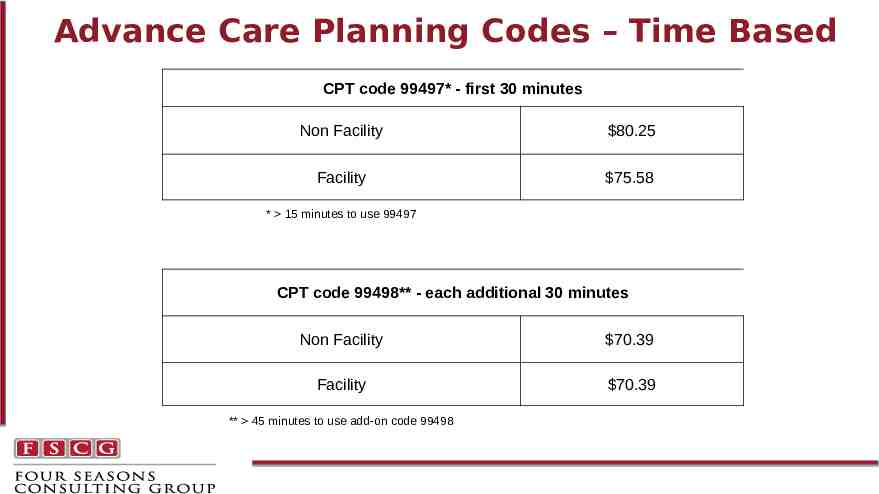
Advance Care Planning Codes – Time Based CPT code 99497* - first 30 minutes Non Facility 80.25 Facility 75.58 * 15 minutes to use 99497 CPT code 99498** - each additional 30 minutes Non Facility 70.39 Facility 70.39 ** 45 minutes to use add-on code 99498
Payment Medicare Administrative Contractors (MACs) will be responsible for local coverage determination Currently no National Determination Coverage Policy which gives time for implementation and experience on use of code 20% co-pay by secondary insurer or patient For primary care physicians can be an add-on to an Annual Wellness Visit with modifier 33 (in this case no 20% co-pay)
Develop a Process Train appropriate personnel Develop a standardized process/template Identify supervising provider Develop internal auditing system Track number month/provide
Scenario 1 74 year old male with advanced heart disease admitted to the hospital with exacerbation of congestive heart failure. Palliative Care consult requested for dyspnea management and goals of care. Physician completes a palliative care consult with recommendations for dyspnea management and has a goals of care conversation The billing is based on a comprehensive history and physical with high medical decision making (Incidentally it takes the provider 50 minutes). In addition, advance directives and goals of care regarding medical treatments is discussed with the patient/family, and a Do Not Resuscitate (DNR) order is placed (25 minutes) What is the correct CPT code for this encounter?
Scenario 1 Billing by intensity - 99223 – Comprehensive history (extended History of Present Illness, complete Review of Symptoms, complete Present Family and Social History – Comprehensive physical – High medical decision making Advance Care Planning (ACP) code – 99497 – Document 25 minutes in Advance Care Planning discussion. Since 15 minutes, allows for 99497 code
Scenario 2 89 year old female with Alzheimer's dementia resides in long term care facility. Patient seen by the Nurse Practitioner the week prior and family meeting set up with daughter. In a family conference room (apart from patient) the Nurse Practitioner spends 50 minutes with daughter and discusses goals of care, Physician Orders for LifeSustaining Treatment (POLST) form, risks and burdens of various medical treatments. POLST form completed. What is the correct CPT code for this encounter?
Scenario 2 99497 – for 1st 30 minutes 99498 – must meet 15 minutes to activate this code, hence since 20 minutes over threshold this code is added No Evaluation/Management code used Prior to Advance Care Planning code, this was an unbillable service Does require Face-to-Face time with surrogate or family
Scenario 3 66 year old female followed by palliative care for management of cancer related pain. On follow up visit in the clinic, physician performs a comprehensive interval history, comprehensive exam, and high medical decision making. Initiation of goals of care coordination occurs and patient immediately directed to continue discussion with the Social Worker. Social Worker spends 60 minutes with discussion and completion of advance directives. What is the correct CPT code for the encounter?
Scenario 3 99215, 99497, 99498 – bill under physician NPI number 99215 – billing by intensity “incident to” codes (99497, 99498) for social Worker time on ACP. Requires appropriate documentation with time component (60 min) for ACP codes. Let’s suppose that instead the Social Worker saw the patient on the following day with same physician present in the clinic and spent 60 minutes Bill as “incident to” using stand alone codes 99497 99498 under physician NPI number
Scenario 4 83 year old female with Chronic Obstructive Pulmonary Disease (COPD) is seen at home for a new visit by palliative care Physician Assistant. A comprehensive history, physical exam, and high medical decision making occurs. This is followed by a 50 minute discussion on goals of care, treatment preferences, and a Do Not Resuscitate Order is obtained. What is the correct CPT code for this encounter?
Scenario 4 Claim submitted under Physician Assistant Name and National Provider Identifier number 99345 – Evaluation/Management code based on intensity 99497 99498 – add on codes with 50 minutes of time documented for Advance Care Planning discussion
Impact of Advance Care Planning Reimbursement More impactful if practicing in clinic setting where Social Worker, Nurse, and Providers are present so can bill under “incident to” rule More impactful if high nursing home census, as Physicians and Providers can bill Advance Care Planning apart from patients who lack capacity
Calculate Impact of Using Advance Care Planning Codes o Increase in revenue by 25,000 per provider/year o Assume 60% new/est visits 20% est/sub o Refer to excel spread sheet and particular care setting # new/initial visits sub/est visits x 99497 reimbursement # new/initial visits sub/est visits x 99498 reimbursement
What about other payers Medicare Advantage – often follows CMS, but need to check with health plan payer Insurers – some already cover
Questions? Use of Advance Planning Codes
Summary o Reimbursement based on care management of advanced illness patients o Implications for a community palliative practice where significant time spent in communication, goals of care discussions, and alignment of care with goals o Opportunities for new partnership, less fragmentation of care, and improved quality for patients and families
Questions? [email protected]