1 Preschool/School Supportive Health Services Program MEDICAID UPDATE

65 Slides380.60 KB
1 Preschool/School Supportive Health Services Program MEDICAID UPDATE TRAINING 2015
2 Agenda New York State Medicaid Program Compliance SSHSP Stakeholders SSHSP Requirements and Provider Responsibilities Medicaid Alerts OMIG Functions and Audit Findings Certified Public Expenditures Interim Claims and Parental Consent Oversight & Monitoring Resources
3 New York State Medicaid Program
4 New York State Medicaid Program Program Goal: To increase access to health care coverage for low income individuals, families and children Medicaid is a program for persons whose income and/or resources are below certain levels. Eligible populations include: children, pregnant women, single individuals, families, and individuals certified blind or certified disabled.
Medicaid Covered Services Medicaid offers a full range of health services for eligible persons. Most Medicaid eligible persons are enrolled in a Medicaid managed care plan and access these services within that plan’s network. Some services are accessed directly through Medicaid fee-for-service (FFS) even when the eligible person is enrolled in a Medicaid managed care plan. SSHSP services are accessed directly through FFS Medicaid. Refer those wishing to apply for Medicaid to the NYS Health Exchange at: http://info.nystateofhealth.ny.gov/contact 5
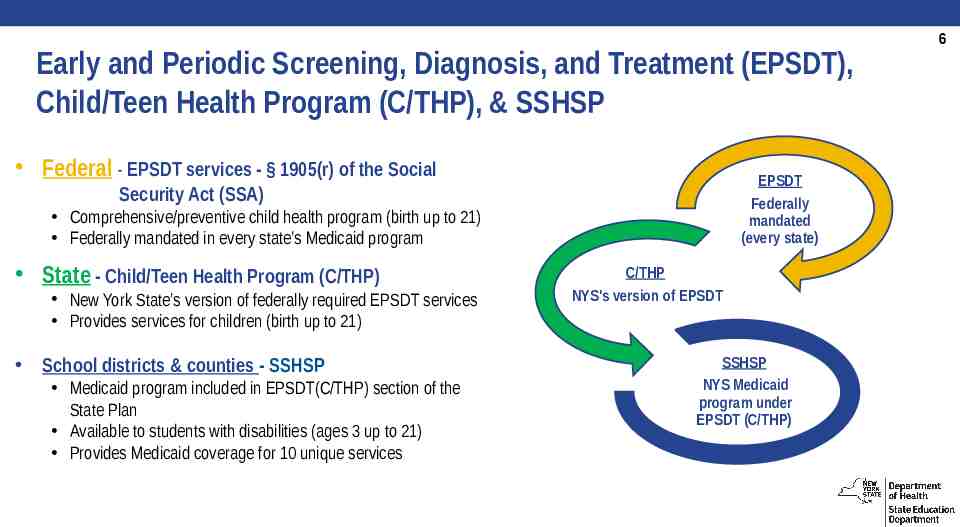
Early and Periodic Screening, Diagnosis, and Treatment (EPSDT), Child/Teen Health Program (C/THP), & SSHSP Federal - EPSDT services - § 1905(r) of the Social EPSDT Federally mandated (every state) Security Act (SSA) Comprehensive/preventive child health program (birth up to 21) Federally mandated in every state’s Medicaid program State - Child/Teen Health Program (C/THP) New York State’s version of federally required EPSDT services Provides services for children (birth up to 21) School districts & counties - SSHSP Medicaid program included in EPSDT(C/THP) section of the State Plan Available to students with disabilities (ages 3 up to 21) Provides Medicaid coverage for 10 unique services C/THP NYS's version of EPSDT SSHSP NYS Medicaid program under EPSDT (C/THP) 6
7 Preschool/School Supportive Health Services Program (SSHSP) A New York State Medicaid program that allows school districts and counties to access federal monies for medically necessary services provided to Medicaid eligible students with disabilities as long as all Medicaid requirements are met.
8 SSHSP Mission To assist school districts and counties in providing quality health care to students with disabilities for certain diagnostic and health support services while accessing Medicaid reimbursement for eligible services and preventing fraud, waste, abuse, and false billing to the Preschool/School Supportive Health Services Program (SSHSP) through compliance with federal and State laws, regulations and guidelines.
9 Compliance
Compliance – SSHS Program History Previous authority to operate the SSHSP in New York State fell under State Plan Amendment (SPA) #92-42. 1998 – Whistleblower filed lawsuits in U.S District Court Federal audits/findings: Justice Department, Office of the Inspector General and the Centers for Medicare and Medicaid Services (CMS) audited New York State’s SSHSP. New York State’s SSHSP was found to be out of compliance with federal and State regulations and guidelines. School districts and counties did not maintain documentation to support Medicaid billing. 10
11 Compliance Agreement Sets down in writing NYS’s commitment: To comply with all federal and State laws and regulations related to Medicaid funding; To ensure policies and practices are modified to achieve compliance; and To remedy the consequences of past practices and policies. Compliance Agreement between NYS and CMS has officially ended. New York State will continue close oversight of the SSHSP and continue to provide Medicaid trainings to ensure continued compliance.
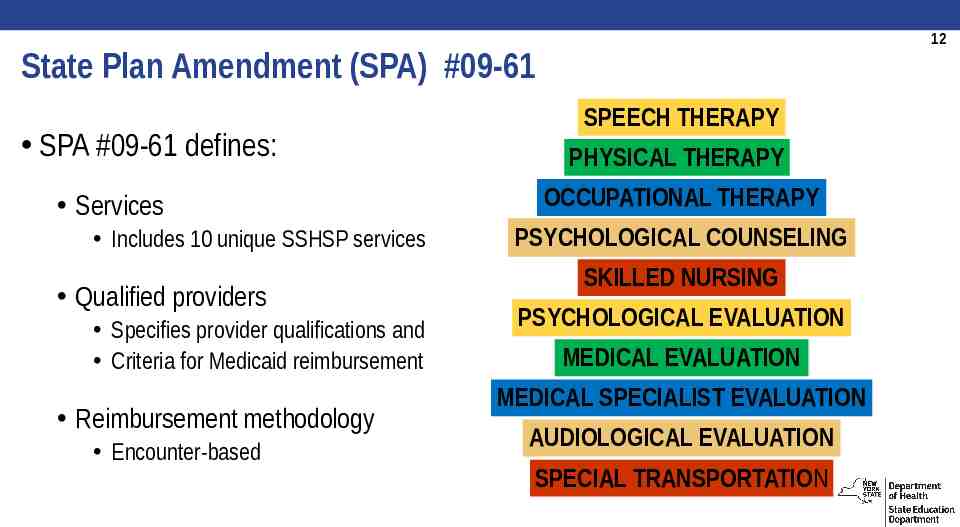
12 State Plan Amendment (SPA) #09-61 SPA #09-61 defines: Services Includes 10 unique SSHSP services Qualified providers Specifies provider qualifications and Criteria for Medicaid reimbursement Reimbursement methodology Encounter-based SPEECH THERAPY PHYSICAL THERAPY OCCUPATIONAL THERAPY PSYCHOLOGICAL COUNSELING SKILLED NURSING PSYCHOLOGICAL EVALUATION MEDICAL EVALUATION MEDICAL SPECIALIST EVALUATION AUDIOLOGICAL EVALUATION SPECIAL TRANSPORTATION
13 SSHSP Stakeholders
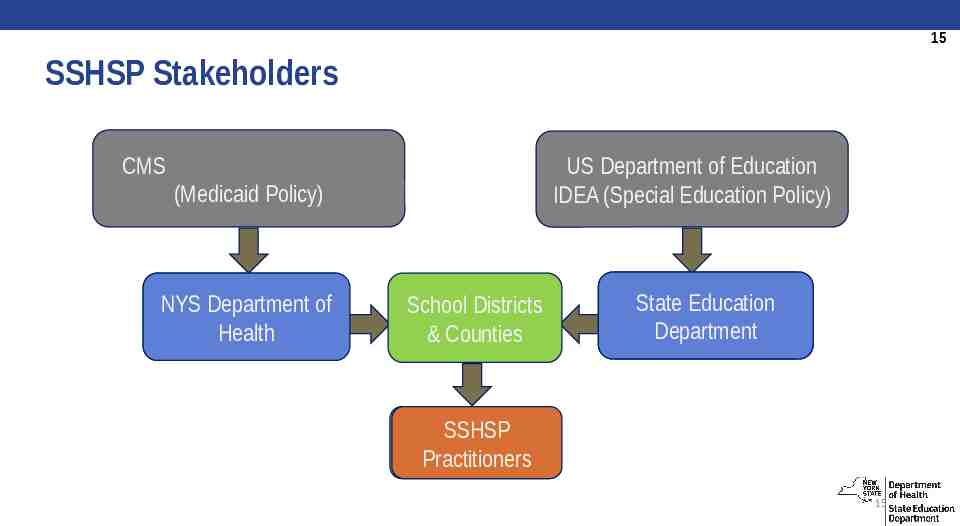
14 SSHSP Stakeholders: Centers for Medicare and Medicaid Services (CMS) U.S. Department of Education (DOE) NYS Department of Health (DOH) NYS Education Department (SED) School Districts & Counties (SSHSP billing providers) SSHSP Practitioners Regional Information Centers (RICs) Central New York Regional Information Center (CNYRIC) Billing Vendors Computer Sciences Corporation (CSC)/eMedNY NYS Office of Medicaid Inspector General (OMIG) Public Consulting Group (PCG)
15 SSHSP Stakeholders CMS US Department of Education IDEA (Special Education Policy) (Medicaid Policy) NYS NYS Department Departmentof ofHealth Health School Districts & Counties State State StateEducation Education Education Department Department Department SSHSP SSHSP Practitioners Practitioners 15
16 SSHSP Requirements and Provider Responsibilities
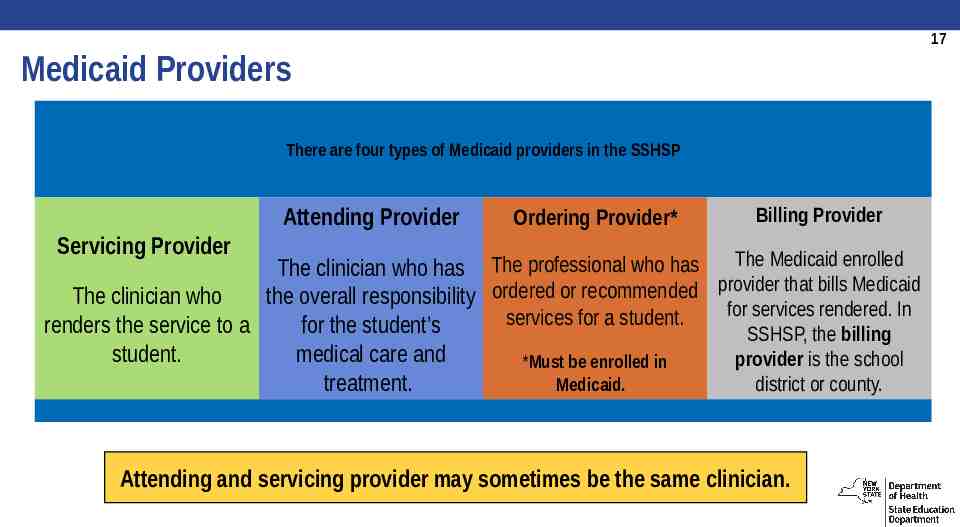
17 Medicaid Providers There are four types of Medicaid providers in the SSHSP Attending Provider Ordering Provider* Billing Provider Servicing Provider The Medicaid enrolled The clinician who has The professional who has provider that bills Medicaid ordered or recommended The clinician who the overall responsibility for services rendered. In services for a student. renders the service to a for the student’s SSHSP, the billing student. medical care and provider is the school *Must be enrolled in Medicaid. treatment. district or county. Attending and servicing provider may sometimes be the same clinician.
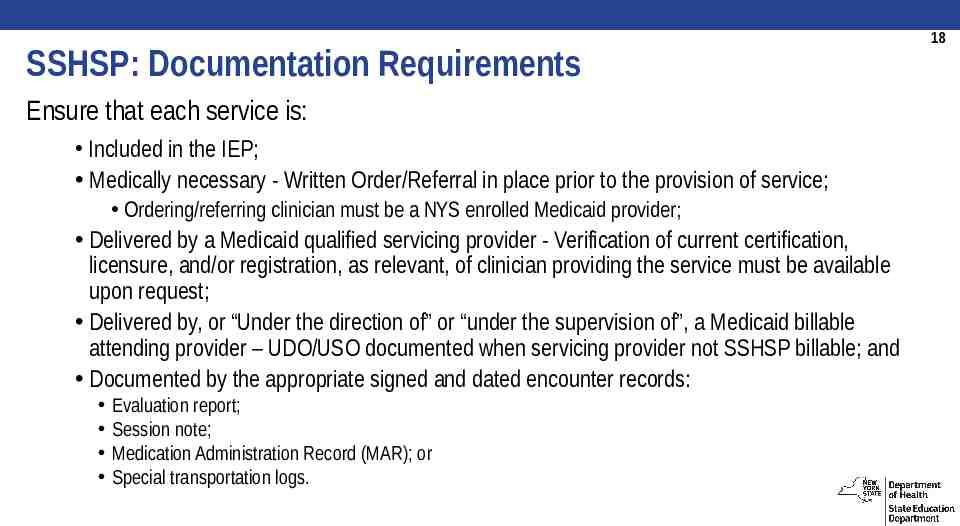
SSHSP: Documentation Requirements Ensure that each service is: Included in the IEP; Medically necessary - Written Order/Referral in place prior to the provision of service; Ordering/referring clinician must be a NYS enrolled Medicaid provider; Delivered by a Medicaid qualified servicing provider - Verification of current certification, licensure, and/or registration, as relevant, of clinician providing the service must be available upon request; Delivered by, or “Under the direction of” or “under the supervision of”, a Medicaid billable attending provider – UDO/USO documented when servicing provider not SSHSP billable; and Documented by the appropriate signed and dated encounter records: Evaluation report; Session note; Medication Administration Record (MAR); or Special transportation logs. 18
Encounter-based Claiming All SSHSP claims are encounter-based. Claims for direct medical services must be supported by documentation as required and must include: Student’s Medicaid client identification number (CIN) and other pertinent demographics; Billing provider’s NPI; Attending provider’s NPI; Ordering/referring provider’s NPI; A valid and appropriate ICD-9 code(s); An appropriate Current Procedural Terminology (CPT) code(s); Procedure code modifier (for PT, OT, and ST claims only); and The number of unit(s). For claims with dates of service October 1, 2015 and after – Free ICD-10-CM official guidelines and code sets online at: http://cms.gov/Medicare/Coding/ICD10/index.html 19
20 SSHSP Administrative Responsibilities For a school district/county (billing provider) to be reimbursed by Medicaid for an SSHSP service, the school district/county must: Have a National Provider Identifier (NPI) and be an enrolled Medicaid provider; Obtain parental consent to bill Medicaid (in accordance with IDEA) prior to claiming; Incur a cost for the service (i.e., the school district/county must not bill Medicaid for a service that is paid partially or in full by Federal funds); Have completed Provider Agreements and Statements of Reassignment for outside contractors (excludes BOCES); The student must be Medicaid eligible (have a Client Identification Number - CIN); Keep affiliation current for attending providers; and Annually certify Electronic Transmitter Identification Number (ETIN)
21 Medicaid Alerts
Medicaid Alert #14-02 International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) Medicaid Alert #14-02 (Issued 5/1/2014) International Classification of Diseases, 10th revision, Clinical Modification (ICD-10-CM) Medicaid claims for SSHSP services must include a valid diagnosis code. The ICD-10 code sets are effective for dates of service on or after October 1, 2015. ICD-10 cannot be used on claims with a date of service prior to October 1, 2015. Written orders/referrals completed prior to October 1, 2015 will remain valid. ICD-10 codes required only on claims (not on supporting documentation). Clinicians can keep informed about changes through the CMS website at: https://www.cms.gov/ICD10/ 22
Medicaid Alert #14-06 Requirement to Use Modifiers on Physical, Occupational, and Speech Therapy Claims Medicaid Alert #14-06 (Issued 10/20/2014) Effective Immediately - Physical, Occupational, and Speech Therapy Claims Now Require Modifiers When two SSHSP Medicaid claims for the same CPT code and service date were processed (e.g., 1 PT & 1 OT), the first claim was paid and the second was denied as duplicate. Starting in Cycle 1952, CNYRIC adds OT/PT/Speech (97000 code) modifiers to all claims based on the servicing professional’s code submitted in the claim. Medicaid Alert #14-04 (Issued 9/15/2014) provided interim method to bill both types under single CPT code, separately document type and units delivered. 23
Medicaid Alert #14-08 Evaluation Clarification for Medicaid Reimbursement Medicaid Alert #14-08 (Issued 11/26/2014) Clarification on SSHSP Medicaid Reimbursement for Evaluations Medicaid reimbursement is available for PT, OT, Speech, and Psychological evaluations ONLY when the IEP includes a recommendation for ongoing services in that therapy type and the evaluation is included in the IEP. The evaluation must also have a written order or appropriate referral dated prior to the evaluation (or an ongoing service order/referral), be documented in a report, be completed by a Medicaid qualified provider, and be included in the student’s IEP. 24
Evaluations: Medicaid Requirements for Reimbursement 25 To be Medicaid reimbursable the school districts/counties must ensure the following requirements are met prior to submitting the claim to Medicaid: A written order/referral (from a Medicaid enrolled provider) dated prior to the actual evaluation is in place; The evaluation is provided by a Medicaid qualified provider; The evaluation is included in the IEP; The evaluation report has been completed; and If it is an initial evaluation for PT, OT, ST, or psychological counseling, the ongoing service in that therapy type is also included in the IEP. NOTE: For psychological counseling evaluations, if the referral is done by an appropriate school official, Medicaid enrollment is waived. Refer to Medicaid Alert #13-04 for more information on Medicaid enrollment of ordering/referring providers.
26 Initial Evaluations: Physical, Occupational, Speech Therapy or Psychological Counseling An initial evaluation is the evaluation that is done: Prior to the development of a student’s first Individualized Education Program (IEP) or Prior to the inclusion of that therapy (PT, OT, ST, or psychological counseling) in the student’s existing or next IEP. An initial evaluation is not Medicaid reimbursable if it is determined that a recommendation for ongoing services in that same therapy type is not needed. NOTE: If an IEP is developed and ongoing services are recommended, the initial evaluation must be reflected in that IEP to be Medicaid reimbursable. Refer to Medicaid Alert #12-03.
27 Re-evaluations: Physical, Occupational, Speech Therapy or Psychological Counseling A re-evaluation is the evaluation that is done after the student has been receiving ongoing services in that same therapy type. Re-evaluations are Medicaid reimbursable even when it is determined that the ongoing service is no longer needed. Example (reimbursable): If a student with an IEP (including ongoing services in speech therapy) is re-evaluated for speech therapy, and it is determined ongoing speech therapy services are no longer needed, that re-evaluation is billable to Medicaid.
28 Evaluations and Re-evaluations: Medical, Medical Specialist, and Audiological Evaluations and re-evaluations (Medical, Medical Specialist, and Audiological) are Medicaid reimbursable without the need for an ongoing service being included in the student’s IEP. All Medicaid requirements must be met in order for the evaluation or reevaluation to be reimbursable. NOTE: To be Medicaid reimbursable, the evaluation or re-evaluation must be included in the IEP.
Medicaid Alert #14-09 Update on RMTS Moment Expiration Medicaid Alert #14-09 (Issued 12/23/2014) Random Moment Time Study (RMTS) Moment Expiration Update Moments assigned to RMTS participants throughout the January-March 2015 quarter are required to be submitted within three (3) school days from the time of the moment. Effective April 1, 2015, moments assigned to RMTS participants are required to be submitted within 48 hours (two (2) school days) from the time of the moment. In addition to the changes in the moment expiration process, RMTS participants (and RMTS Coordinator) will no longer be notified in advanced of a moment, but rather, will receive notification at the exact time of their moment. 29
30 Medicaid Alert #15-01 SPA Approvals Medicaid Alert #15-01 (Issued 1/16/2015) Medicaid State Plan Amendments for Certified Public Expenditures have been Approved State Plan Amendments (SPA) #11-39-A (school districts) and #11-39-B (counties) have been approved. SPA #09-61, which provides for interim fee-for-service claiming, remains in effect. After the school year is over, the Certified Public Expenditure (CPE) process will adjust that interim Federal Medicaid reimbursement to reflect the district’s Medicaid allowable costs for providing SSHSP services. Any district billing for the SSHSP services in 2011-12 school year or thereafter must complete this CPE cost settlement process.
31 Medicaid Alert #15-02 Clarification of Medicaid Reimbursement for Nursing Services Medicaid Alert #15-02 (Issued 3/04/2015) Clarification on Medicaid reimbursement for nursing services Depending on the nature of the nursing services that are required, the documentation in the student’s IEP could, as appropriate to the individual student’s needs, be included as follows: The IEP may specify school health services or school nurse services as a related service with further clarification under the column “Service delivery recommendations” that such services are “skilled nursing services.” Alternatively, as appropriate to the student’s need for certain skilled nursing services, IEP recommendations for skilled nursing services could be noted as “supplementary aids and services.”
32 Medicaid Alert #15-03 Revalidation of Enrollment Medicaid Alert #15-03 (Issued 3/23/2015) NYS DOH Medicaid Provider Revalidation Process The federal Affordable Care Act requires that all state Medicaid providers, including SSHSP enrolled Medicaid billing providers, revalidate their Medicaid enrollment information. Please note that the SSHS program is not exempt from this process and failure to respond will result in the termination of your enrollment in the SSHS program and your school district or county will be unable to submit claims for Medicaid reimbursement. Your school district or county is required to complete this Medicaid enrollment revalidation process within 90 days of the date of the NYSDOH letter or no later than May 22, 2015.
33 Office of the Medicaid Inspector General (OMIG) Functions and Audit Findings
Office of the Medicaid Inspector General (OMIG) Mission: To enhance the integrity of the New York State Medicaid program by preventing and detecting fraudulent, abusive, and wasteful practices within the Medicaid program and recovering improperly expended Medicaid funds while promoting high-quality patient care. The Office of the Medicaid Inspector General (OMIG) is an independent entity created within the New York State Department of Health to improve and preserve the integrity of the Medicaid program by conducting and coordinating fraud, waste, and abuse control activities for all State agencies responsible for services funded by Medicaid. OMIG is: The Medicaid auditing agency; Responsible for managing the OMIG Compliance Program; and Responsible for maintaining the Medicaid Termination and Exclusion Lists. 34
35 OMIG Compliance Program Social Services Law §363-d 18 NYCRR Part 521 Ensures Medicaid providers establish systemic checks and balances to detect and prevent inaccurate billing and inappropriate practices in the Medicaid program All persons, providers or affiliates claiming, ordering or receiving payments in excess of 500,000 (gross) from the Medical Assistance Program Annual recertification required
Medicaid Terminations and Exclusions (Individuals or Entities) The Medicaid program wants to ensure that the best medical professionals participate in the Medicaid program. When the Medicaid program finds good reason that a provider should no longer be eligible to participate, they are placed on a list of excluded providers. 36
Medicaid Terminations and Exclusions (Individuals or Entities) Prior to adding new staff members, employers should check to see if prospective employees have been excluded from Medicaid. An individual excluded from the Medicaid program may be qualified under NYS law to provide services, but no federal/State health reimbursement can be claimed under any program To access this list, click on the link below, and read the explanation and disclaimers regarding the list of terminations and exclusions: http://www.omig.ny.gov/information-about-medicaid-terminations-and-exclusions 37
Medicaid Terminations and Exclusions (Individuals or Entities) To make it easier to perform such a check, OMIG set up a dedicated service to check the status of any exclusion. NYS Exclusion List: http://www.omig.ny.gov/index.php/fraud/medicaid-terminations-andexclusions Federal Exclusion List: http://oig.hhs.gov/exclusions/index.asp Providers with questions about exclusions and terminations should call NYS OMIG at 518-486-9956. 38
39 OMIG SSHSP Audit - 2013 OMIG uncovered the following during their 2013 audit of the SSHSP: Incomplete documentation of UDO/USO; Billing for individual services when they are not included on the IEP; Incorrect billing of speech evaluations; Incomplete documentation of skilled nursing services involving medication administration; Billing for round trip special transportation when documentation only indicated one-way special transportation on the date of service.
40 OMIG – Fighting Fraud, Waste and Abuse Health care professionals are on the frontlines in fighting fraud. Ways to keep in touch with OMIG: Join the OMIG mailing list: http://www.omig.ny.gov/omig-email-list-subscriptions Follow OMIG on Twitter: https://twitter.com/nysomig Contact OMIG: http://www.omig.ny.gov/index.php/information/contact-us#contact
41 Certified Public Expenditures
42 Certified Public Expenditures (CPEs) The CPE reimbursement methodology is an annual cost reconciled and settled reimbursement methodology. CPE cost settlements based on school year (July 1st to June 30th) Allows NYS to request additional federal funding for costs not completely covered by current Medicaid reimbursement. Public Consulting Group (PCG) is the Department of Health’s contractor who will assist with the implementation of the CPE reimbursement methodology.
43 Certified Public Expenditures (CPEs) The major components of the CPE reimbursement methodology are: Time spent by practitioners delivering Medicaid reimbursable services (Random Moment Time Study – RMTS) Actual costs including employee salaries, fringe benefits, contract costs, and equipment purchases and maintenance (reflected in annual cost reports); and Interim Medicaid reimbursement received from encounter-based billing.
44 Random Moment Time Study (RMTS) Purpose of the Time Study: The random moment time study (RMTS) is used to determine the amount of time (and cost) spent on various activities. The RMTS is required as part of the annual cost settlement process. This is one of the most crucial reimbursement determinants used by the NYS Department of Health.
45 Random Moment Time Study (RMTS) The RMTS includes the distribution of 2,827 moments to participants within cost pool on a quarterly basis. Moments are randomly assigned to participants at the start of the quarter. The RMTS is an ongoing, quarterly process. each Moments are not generated for the summer quarter (no moments sent July-September); instead, an average of the other three quarters is used. The RMTS is NOT a management tool used to evaluate staff activities or performance. The results of the time study will ONLY be used for cost allocation purposes. What is your role as an RMTS participant? Participants are responsible for responding to each and every moment they receive with a detailed and accurate submission.
46 Random Moment Time Study (RMTS) All moment notifications are sent to participants via e-mail from [email protected]. Participants no longer receive an advance notice of their upcoming moment(s). After the moment has occurred, participants will log on to the secure website using the link provided in the initial e-mail. Participants are asked to respond to a series of questions describing the activity performed at the time of the moment. Participants have 48 hours to respond to each moment.
47 Random Moment Time Study (RMTS) Remind Your RMTS Participants! A moment represents a minute in time. If there is not enough information provided in a moment response, PCG will follow up and request that the moment is resubmitted with a more detailed response. The participant will view a confirmation page once the moment is successfully completed. If the participant is not brought to the confirmation page, the moment may not have been submitted successfully. Participants are expected to respond to each assigned moment. The RMTS is an important and required part of the annual cost settlement process.
48 Cost Settlement Process What is cost based reimbursement? A cost based reimbursement methodology determines the actual cost of delivering SSHSP services to special education students. Cost based reimbursement ensures that reimbursement for the delivery of medical services reflects the actual cost of providing the service. Districts and counties are responsible for submitting the Annual Medicaid Cost Report in order to determine their allowable cost settlement.
49 Cost Settlement The Department has submitted a certified public expenditure (CPE) claim to the Centers for Medicare and Medicaid Services (CMS) for the 2011-12 and 2012-13 school years. The retroactive CPE claim submitted for the 2011-12 and 2012-13 school years included “rest-of-state” school districts and counties and did not meet the threshold for gainsharing. Social Services Law (Article VII language) as part of the 2014-15 Enacted State Budget includes gain sharing provisions without a threshold beginning with the 2015-16 school year cost report.
50 Interim Claims and Parental Consent
51 Interim Claiming Interim claiming for SSHSP services Claims submitted by schools/counties to Medicaid for reimbursement; and Use the encounter-based billing methodology Benefits of increasing interim claims: Increase interim Medicaid dollars received by SSHSP providers; Increase overall reimbursement for the SSHS Program; Ensure program integrity; Provides timely funding soon after expense incurred; and Allows time for resubmissions. Best practice in increasing the amount of interim claims submitted: Submit claims as soon as all Medicaid requirements are verified.
52 Parental Consent School districts and counties must obtain a one-time written consent from the parent; and Annually, provide parents with a written notification of their rights and the opportunity to withdraw consent. Medicaid may not be billed for SSHSP services furnished to a student without a separate signed parental consent that meets IDEA and FERPA requirements. Information on parental consent can be found online at: http://www.p12.nysed.gov/specialed/publications/parentalconsent-medicaid-July2013.htm FYI – This is a Federal Educational Rights and Privacy Act (FERPA) requirement.
Interim Claiming, CPEs, and Parental Consent Not having a Parental Consent form on file results in no Medicaid reimbursement for that student. Every student not having a Parental Consent form on file decreases the amount of interim claiming (Medicaid funding) a school district/county may do. The amount of interim claiming done by each school district/county directly relates to CPE reimbursements. FYI – Interim claiming is the foundation of the CPE process; CMS and the State expect participating SSHSP billing providers to submit interim claims for eligible students. Every effort should be made to ensure that lack of Parental Consent is not a barrier to submission of interim claims. 53
54 Parental Consent Increase Parental Consent form completions and increase interim claiming Use every face-to-face with parent as an opportunity to get Parental Consent signed; Parent/teacher conferences; Clinician/parent meetings; New student enrollments; and Home visits. Other strategies?
55 Oversight and Monitoring
56 Oversight & Monitoring of the CPE Reimbursement Methodology Goal of New York State’s oversight and monitoring of the CPE reimbursement methodology: To provide adequate fiscal monitoring of both the contractor (Public Consulting Group) and the providers (school districts/counties) to ensure that payments are in compliance with efficiency and economy as required under the Social Security Act section 1902(a)(30)(A).
57 Oversight & Monitoring of the CPE Reimbursement Methodology Adequate oversight and monitoring is a federal requirement. Monitoring requirements address: Interim claim submission; Medicaid cost-per-service; Time study processes (RMTS and 100% Time Study); and Highlights school/county outliers.
58 Oversight & Monitoring of the CPE Reimbursement Methodology Monitoring process and tools are designed to: Detect improper payments; Ensure providers are properly submitting interim claims; Ensure Medicaid costs-per-service are reasonable; Prevent waste through the recovery of overpayments; and Identify suspected cases of fraud or abuse and refer to the OMIG for follow-up.
59 Oversight & Monitoring of the CPE Reimbursement Methodology The following districts/counties will be reviewed annually: NYC School District, Buffalo City School District, Rochester city School District, Yonkers City School District, and Syracuse City School District; An additional 30 SSHSP Providers (25 districts/5 counties); and Any district found to be an outlier - interim claim submission or in any other area.
60 Resources
61 Resource: Medicaid-In-Education Website http://www.oms.nysed.gov/medica id/ Sign up on the LISTSERV – Get updates automatically.
62 Resources: Support Services Regional Information Centers (RICs) Medicaid 101 Training Documentation Training Direct support http ://www.oms.nysed.gov/medicaid/contacts/ri c contacts.html Random Moment Time Study (RMTS) and Annual Cost Reporting: PCG Hotline: 866-912-2974 [email protected]
63 Compliance – Documentation Training Documentation training is conducted on site for schools/counties by RICs Initiated as feature of mandatory trainings; may be provided on request Supports in-house compliance program Assist in identification of proper documentation for interim claiming Not an audit – identifies best practices improving documentation compliance Areas of common concern where training has focused: Under the Direction or Supervision of (UDO/USO)- necessary activities Written Orders - elements are required on the order/referral Session Notes- what needs to be included on a session note
64 Resources: State Contacts NYS DOH - SSHSP Medicaid Policy and Medicaid Claiming Questions DOH 518-473-2160 DOH SSHSP Mailbox: [email protected] SED - Medicaid in Education SED 518-474-7116 [email protected]
Resources: Compliance Officer Robert Jake LoCicero; Esq. Deputy Director of Administration Corning Tower – Room 2863 Albany, New York 12237 Telephone: (518) 474-9868 65