Health Economics Workshop: Review of concepts Monisha Sharma, PhD

18 Slides601.59 KB
Health Economics Workshop: Review of concepts Monisha Sharma, PhD International Clinical Research Center (ICRC) University of Washington
Outline Measuring costs Valuing costs Fixed vs variable Perspective Discounting
Uses of cost data Priority setting for new interventions or introducing new technologies, drugs, vaccines Resource requirements and advocacy Financial planning and budgeting Economic evaluation/Improving technical efficiency
Measuring costs Type of costing you conduct depends on your goal Estimating intervention costs from an RCT Bottom-up costing (microcosting) Quantify and cost each input consumed in preventing or treating disease Usually combined with either ingredients-based costing or activity-based costing Estimating efficiency of a currently implemented intervention Gross‐costing (top‐down) Estimate cost for a given volume of patients by dividing the total cost by the volume of service use Usually combined with ingredients-based costing In reality you will likely use a mix of approaches 4
Estimating costs Direct Health Care Costs Hospital, doctor’s office Medications, procedures, tests, healthcare provider cost Direct Non‐Health Care Costs Transportation, childcare, out of pocket expenses Time Costs Patient time waiting for and receiving care, (lost work time related to intervention) Patient recovery time, lost productivity (indirect costs)
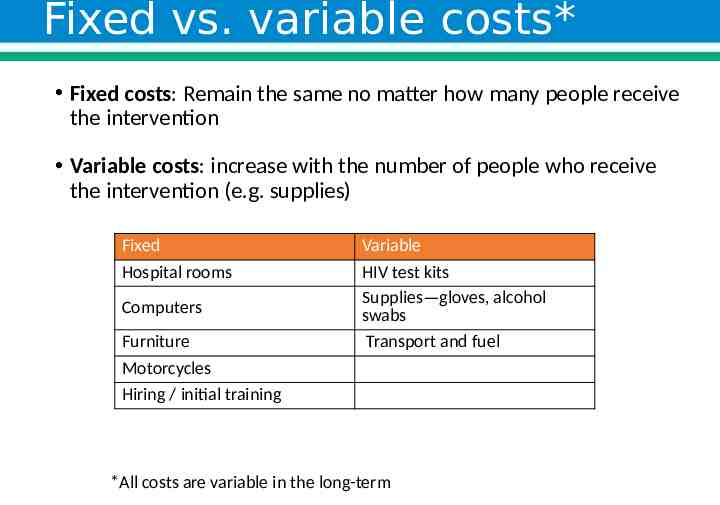
Fixed vs. variable costs* Fixed costs: Remain the same no matter how many people receive the intervention Variable costs: increase with the number of people who receive the intervention (e.g. supplies) Fixed Hospital rooms Computers Furniture Motorcycles Hiring / initial training Variable HIV test kits Supplies—gloves, alcohol swabs Transport and fuel *All costs are variable in the long-term
Perspective Payer perspective Only costs paid by the organization implementing the program (eg Ministry of Health, private insurance company, NGO) are included Societal perspective All costs in incurred or saved by the program are included, regardless of who experiences them This perspective includes: patient time waiting and receiving care, transport costs, and lost wages resulting from sick days related to the intervention. Which perspective should you use? Depends who is using the cost data or CEA results. Governments are often interested in the costs incurred by society. Private insurers may only be interested cost incurred by the company.
Valuing costs Depending on the objective, use economic or financial costs. Budget impact analyses use financial costs. Economic evaluations (eg cost-effectiveness analyses) should include all economic consequences, not just financial costs Eg volunteer time or donated materials or space Price is 0 (financial cost) but economic cost is the value of the service that could be going to another intervention/activity, eg the wage that a volunteer could be making or rental cost of donated space (opportunity costs) What is an opportunity cost? The cost of the next best thing you would have done with the time/resources
Opportunity costs Opportunity costs The value of the best alternative foregone Tradeoffs (opportunity costs) are not always explicit but always exist. For example: opportunity cost of a male circumcision intervention is an alternative health intervention you could have implement with the resources What is your financial cost for attending this lecture? What is you opportunity cost?
Discounting Time Preference: If competing programs have incur costs at different times in the future, we need to have a method to adjust these cost data to allow for comparison To account for time preference, we discount future costs and benefits to a present value
Discounting Health benefits and costs related to an intervention occur at different points in time. But society has a preference for interventions where benefits occur sooner. Discounting Adjusts future health benefits and costs to present value Reflect opportunity for investment (common discount rate is 3%: standard rate of return on long-term riskless investments) Costs and health outcomes are discounted at the same rate.
Discounting costs: present value calculation 𝐹𝑢𝑡𝑢𝑟𝑒 𝑣𝑎𝑙𝑢𝑒 𝑃𝑟𝑒𝑠𝑒𝑛𝑡 𝑣𝑎𝑙𝑢𝑒 𝑛 (1 𝑟 ) What is the present value of 5,000 received 10 years from now? Present value calculator: https://dqydj.com/present-value-calculator-and-present-v alue-formula/ Answer: 3,720.47
Standard discount rates US Panel on Cost Effectiveness in Medicine 3% costs and benefits 5% and 0% in sensitivity analyses United Kingdom NICE guidance: 3.5% for costs and benefits
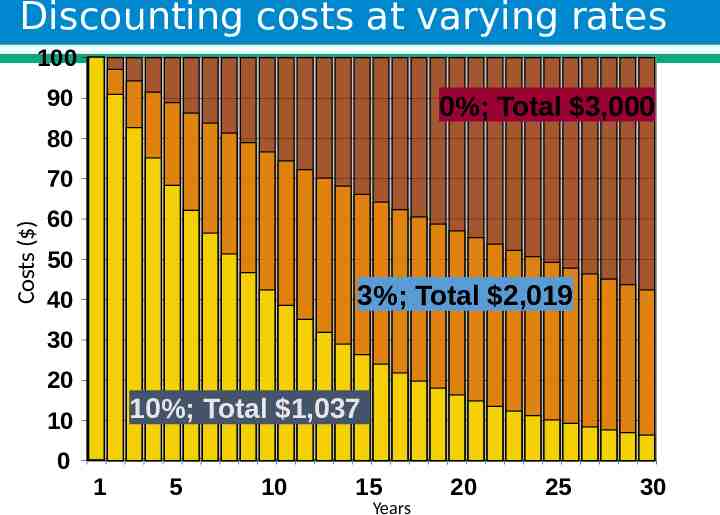
Discounting costs at varying rates 100 90 0%; Total 3,000 80 Costs ( ) 70 60 50 3%; Total 2,019 40 30 20 10%; Total 1,037 10 0 1 5 10 15 Years 20 25 30
Valuing capital costs Vehicles, computers, buildings Usually purchased at the start of an intervention/program Generally assumed to have 5 years of useful life Annualized over their years of useful life and discounted at 3% annually Implications on cost analysis: Should you use purchase price of equipment or replacement price?
Annualizing start up and capital costs Standard assumptions: Vehicles & equipment are used for 5 years before they are replaced Staff hiring and training happens every 5 years b/c of staff turn over Advantage of using standard assumptions: Your costing is comparable with other analyses in the literature You can compare your program costs head-to-head with costings of other programs Disadvantage: May not be accurate in your setting. Eg. Vehicles in developing settings may be used for much longer than 5 years. Staff turnover may be more frequent than 5 years. Choice of assumptions depends on goal of costing
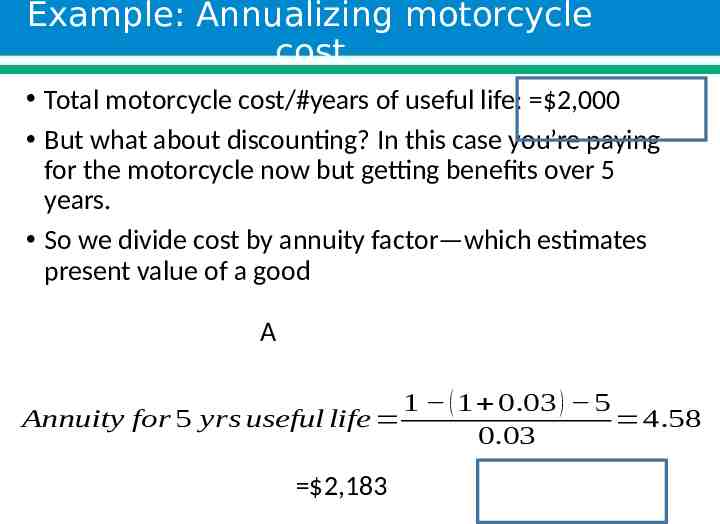
Example: Annualizing motorcycle cost Total motorcycle cost/#years of useful life: 2,000 But what about discounting? In this case you’re paying for the motorcycle now but getting benefits over 5 years. So we divide cost by annuity factor—which estimates present value of a good A 1 ( 1 0.03 ) 5 Annuity for 5 yrs useful life 4.58 0.03 2,183
Thank You! Email: [email protected]