ePMA How big should the team be? Mick Heaton, EPR Programme Manager
20 Slides307.88 KB
ePMA How big should the team be? Mick Heaton, EPR Programme Manager Libby Woodcock, EPR Training & Implementation Manager
Our Voyage of Discovery Stage 1 – Go Live Preparation - 2011 8 months process mapping, clinical engagement, UAT and live prep Clinical Safety sign off by Lead Responsible Officer– Oct 2011 Project Manager, Support, 2 Pharmacy Leads (without backfill) Worked in close collaboration with Supplier Advanced Paediatric Nurse Prescriber Lead – started Oct 2011 First site in UK live on Medchart - November 2011
Open Seas Stage 2 – Royal Oldham Medicine Pilot - 2012 2 month pilot on18-bed Rehab ward Supported 4 four drug rounds with 3 staff – labour intensive Self support and training undertaken by Pharmacy 10 medical pilot wards of increasing patient flow/complexity added Doctor changeover and on call presented particular problems ePMA Lead Nurse replaced by Libby - further nurse added October MAU live November Struggled to provide 24 hour cover needing Supplier support Floyd Unit at Rochdale next – multiple sites brought new challenges
Waters Get Choppy Stage 3a – Business Case Negotiations - 2013 Completed pilot November ’12 with compelling rollout business case Agreed to recruit at risk and rollout to Fairfield Hospital Contract/permanent staff recruited and trained – brought challenges 8 months review of ROI at Trust Board – hard cash vs time to care Fairfield rollout stalled following training - Clinicians at arms Interim approval to roll out at Oldham only & recalculate benefits Business Case finally approved in July 2013 with proviso that 6 nurses released for project and ward-based Phlebotomy removed
Iceberg Abandon Ship! Stage 3b- Royal Oldham Surgery and Maternity - Feb to August 2013 Integrated Discharge Summary and Radiology Order Comms added Surgical rollout at ROH completed on time Theatres pulled at 11th hour due to Anaesthetist refusal Led to prolonged transcription issues with increasing clinical risk Maternity users trained but rollout cancelled because of Theatres. Emergency Action plan for Theatres – proves most challenging area
Back on Course .Storms Ahead! February to December 2013 Stage 4 – Rollout 1 Ward at week at pace Team of 6 staff – still problems covering 24 hour areas Rolled out to Medicine at North Manchester Theatres/ICU – Royal Oldham – challenging required most support Rolled out to Fairfield Medicine Wards Winter Pressures/Process Issues in NMGH Surgery – backed out CSC announcement– Trust had exceeded scalability limitations
Cruising Home November 2014 to Present Implemented Medicines Reconciliation and scalable release Award from NHS England - strengthened deployment team & BAU Rollout at 2 wards per week starting ID at North Manchester Fairfield Surgical Areas, Theatres and Critical Care on time Rochdale Medicine, Surgery and Theatres on time North Manchester Surgical Wards, Theatres & Critical Care to plan Phase completed - 77 Wards – 900 beds – 5300 users - no paper Largest Medchart deployment in the World so far
Maiden Voyage - Lessons Learned Minimize use of dual systems Remove transcription steps Process map at ward level Consider all patient pathways Multiple sites work differently 24 hour support in MAU, Critical Care, Theatres, Maternity Strengthen BAU from go live Need Lead for each staff group Every Site and Division Don’t train too early TOR – Lead Action & Decide IM&T keep within their TOR Time to care is not cash release Consider Winter Pressures Consider Locums and Bank Consider Change of House Consider Ward Reconfiguration Carefully consider Theatres IT/Clinical Trainer mix works best You can’t please everyone!
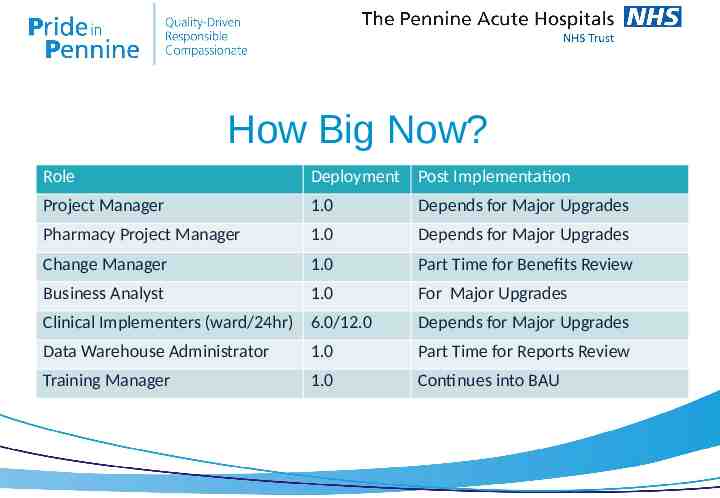
How Big Now? Role Deployment Post Implementation Project Manager 1.0 Depends for Major Upgrades Pharmacy Project Manager 1.0 Depends for Major Upgrades Change Manager 1.0 Part Time for Benefits Review Business Analyst 1.0 For Major Upgrades Clinical Implementers (ward/24hr) 6.0/12.0 Depends for Major Upgrades Data Warehouse Administrator 1.0 Part Time for Reports Review Training Manager 1.0 Continues into BAU
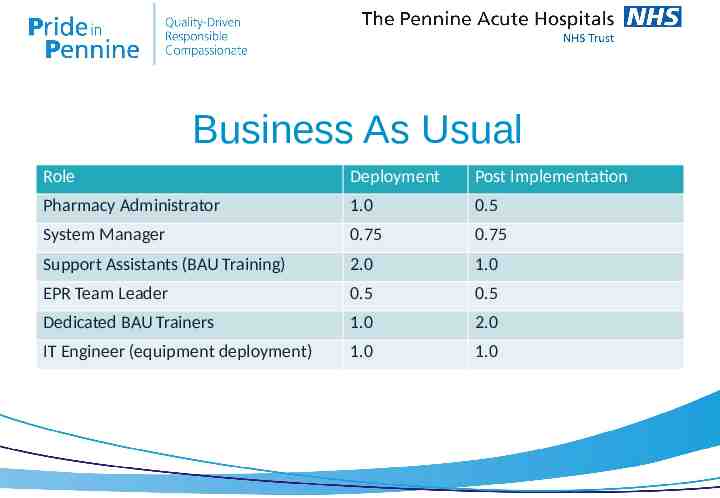
Business As Usual Role Deployment Post Implementation Pharmacy Administrator 1.0 0.5 System Manager 0.75 0.75 Support Assistants (BAU Training) 2.0 1.0 EPR Team Leader 0.5 0.5 Dedicated BAU Trainers 1.0 2.0 IT Engineer (equipment deployment) 1.0 1.0
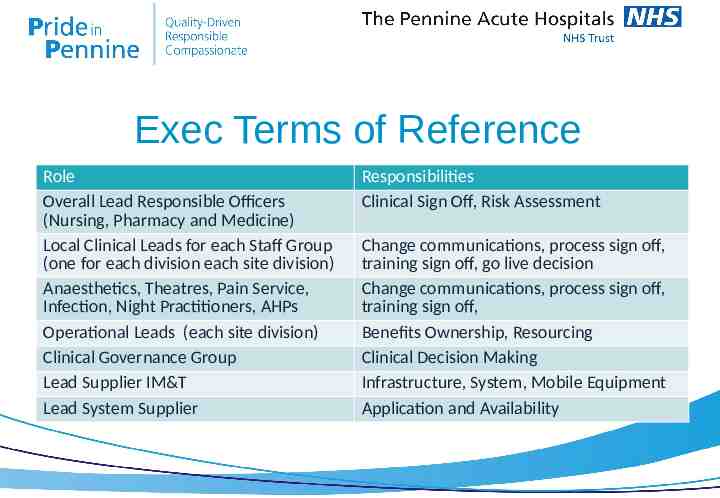
Exec Terms of Reference Role Overall Lead Responsible Officers (Nursing, Pharmacy and Medicine) Local Clinical Leads for each Staff Group (one for each division each site division) Anaesthetics, Theatres, Pain Service, Infection, Night Practitioners, AHPs Operational Leads (each site division) Clinical Governance Group Lead Supplier IM&T Lead System Supplier Responsibilities Clinical Sign Off, Risk Assessment Change communications, process sign off, training sign off, go live decision Change communications, process sign off, training sign off, Benefits Ownership, Resourcing Clinical Decision Making Infrastructure, System, Mobile Equipment Application and Availability
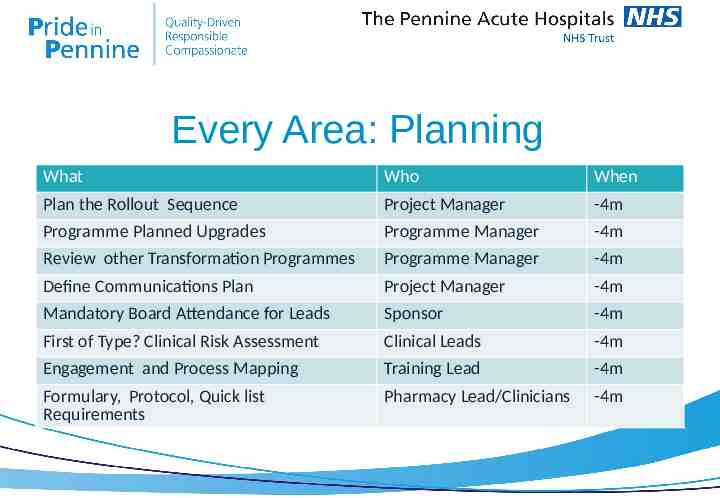
Every Area: Planning What Who When Plan the Rollout Sequence Project Manager -4m Programme Planned Upgrades Programme Manager -4m Review other Transformation Programmes Programme Manager -4m Define Communications Plan Project Manager -4m Mandatory Board Attendance for Leads Sponsor -4m First of Type? Clinical Risk Assessment Clinical Leads -4m Engagement and Process Mapping Training Lead -4m Formulary, Protocol, Quick list Requirements Pharmacy Lead/Clinicians -4m
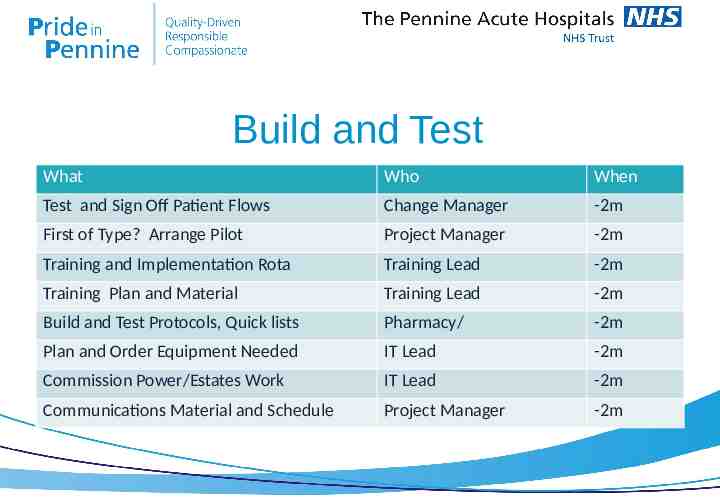
Build and Test What Who When Test and Sign Off Patient Flows Change Manager -2m First of Type? Arrange Pilot Project Manager -2m Training and Implementation Rota Training Lead -2m Training Plan and Material Training Lead -2m Build and Test Protocols, Quick lists Pharmacy/ -2m Plan and Order Equipment Needed IT Lead -2m Commission Power/Estates Work IT Lead -2m Communications Material and Schedule Project Manager -2m
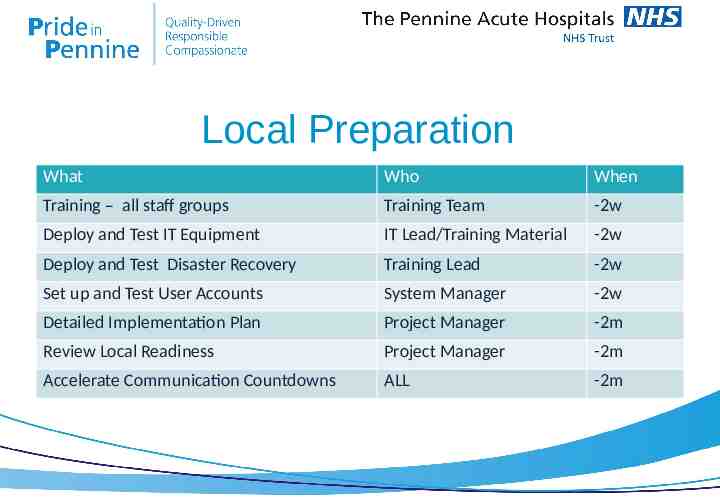
Local Preparation What Who When Training – all staff groups Training Team -2w Deploy and Test IT Equipment IT Lead/Training Material -2w Deploy and Test Disaster Recovery Training Lead -2w Set up and Test User Accounts System Manager -2w Detailed Implementation Plan Project Manager -2m Review Local Readiness Project Manager -2m Accelerate Communication Countdowns ALL -2m
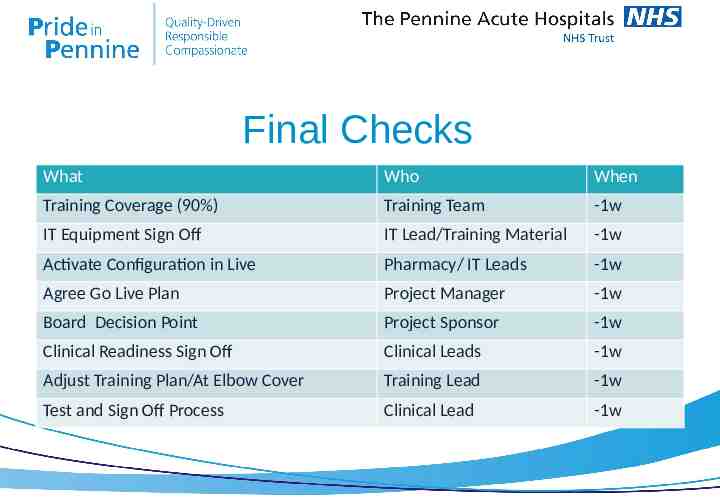
Final Checks What Who When Training Coverage (90%) Training Team -1w IT Equipment Sign Off IT Lead/Training Material -1w Activate Configuration in Live Pharmacy/ IT Leads -1w Agree Go Live Plan Project Manager -1w Board Decision Point Project Sponsor -1w Clinical Readiness Sign Off Clinical Leads -1w Adjust Training Plan/At Elbow Cover Training Lead -1w Test and Sign Off Process Clinical Lead -1w
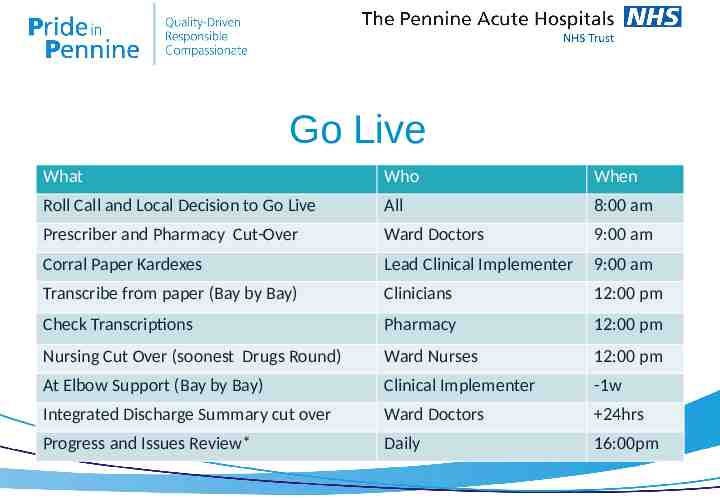
Go Live What Who When Roll Call and Local Decision to Go Live All 8:00 am Prescriber and Pharmacy Cut-Over Ward Doctors 9:00 am Corral Paper Kardexes Lead Clinical Implementer 9:00 am Transcribe from paper (Bay by Bay) Clinicians 12:00 pm Check Transcriptions Pharmacy 12:00 pm Nursing Cut Over (soonest Drugs Round) Ward Nurses 12:00 pm At Elbow Support (Bay by Bay) Clinical Implementer -1w Integrated Discharge Summary cut over Ward Doctors 24hrs Progress and Issues Review* Daily 16:00pm
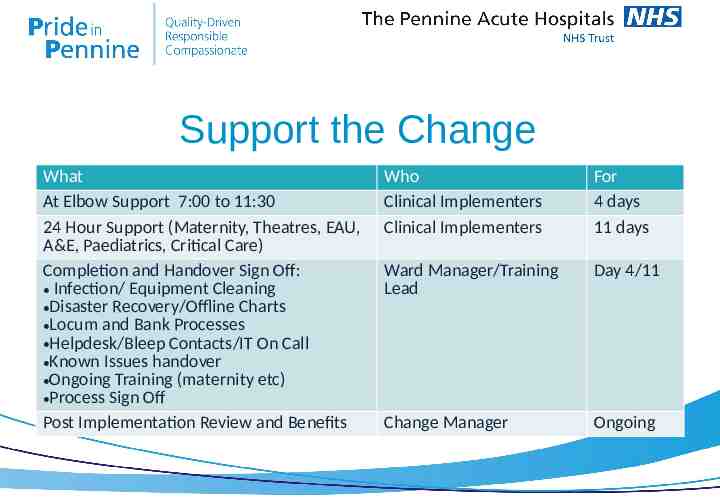
Support the Change What At Elbow Support 7:00 to 11:30 24 Hour Support (Maternity, Theatres, EAU, A&E, Paediatrics, Critical Care) Completion and Handover Sign Off: Infection/ Equipment Cleaning Disaster Recovery/Offline Charts Locum and Bank Processes Helpdesk/Bleep Contacts/IT On Call Known Issues handover Ongoing Training (maternity etc) Process Sign Off Post Implementation Review and Benefits Who Clinical Implementers Clinical Implementers For 4 days 11 days Ward Manager/Training Lead Day 4/11 Change Manager Ongoing
What Could Possibly Go Wrong? Infection Outbreak Medical Emergency Staff Sickness (esp Ward Mgr) Unplanned Staff Groups Revert to Paper – 1st unsupported weekend flashpoint PAS errors – Drugs Ceased! Locums arrive at all hours Interface issues Performance dips at transcription System down at transcription Wi-Fi black spot at Bed 15, Bay 2 Nurses refuse to Withhold Drugs Localised Printing Issues Incorrect User Set Up Anomalies: “ but I do it that way” “I didn’t know anything about this!” “Didn’t no one tell you about the transfers to MR at Salford”? “I don’t have time to do this!” “Are you making me redundant!”
What Next? Discharge Summary process change Series of Patch upgrades to fix known issues Phase 2 Complex Prescribing - Maternity Live through September Oncology and Community Stepdown beds - October Paediatrics and Neonates – November/December Med Reconciliation into the Discharge Summary – November Preadmission prescribing for MAU and Surgery Phase 3 A&E Pilot, Outpatient Pilot – CSC Roadmap Delays Oxygen, Infusions, Chemo, Listening into Action, supplementary charts, ipad version
ANY QUESTIONS? Mick Heaton, EPR Programme Manager Libby Woodcock, EPR Training & Implementation Manager