Ambulatory CDI on a Poor Man’s Budget Rita Fields, BSN, RN, CCDS


23 Slides286.59 KB
Ambulatory CDI on a Poor Man’s Budget Rita Fields, BSN, RN, CCDS Lori Ganote, MSN, RN, CCDS 1
How Did It All Begin? Resource Council Meeting – Goal was to establish outpatient CDI – Move from financial CDI program to quality-based CDI program Recognition of need – Attending meetings related to ambulatory CDI – Collaboration with insurance company – Risk adjustment audits – HCC concept discussed at local meeting – ACDIS conference kept hearing outpatient CDI – HCCs, VBP, risk adjustment became familiar terms
Outpatient CDI vs Ambulatory CDI Executive director separates the two – Ambulatory CDI: physician practice side – Outpatient CDI: hospital side Decision made to begin with ambulatory CDI – Audits showed some physician practices had low RAF scores – Documentation was not capturing HCCs – Chronic conditions requiring yearly documentation How could inpatient CDI help?
HCCs: Why Do They Matter? Hierarchical Condition Categories (HCC) – Risk adjustment methodologies: Insurance companies receive reimbursement for the illness burden of a particular patient Some health plans in turn share this increased revenue with providers Using just CMS-HCCs should capture at least 90% of the risk adjustment for inpatient and outpatient programs – Used to determine reimbursement for various Medicare plans – Addresses predominately elderly population (65 and over) – Captured by claims submitted inpatient and outpatient
HCC Impact Risk Adjustment Factor (RAF) scores to predict future healthcare costs for plan enrollees Adjust payment based on the health status and demographic characteristics of the enrollee Chronic conditions Age Gender Institutionalization status Medicaid status Current reason for Medicare eligibility CMS pays participating health plans a monthly capitation payment based on CMS-HCCs 5
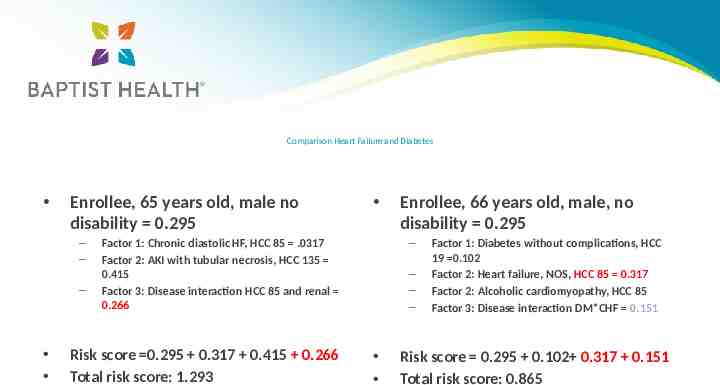
Comparison Heart Failure and Diabetes Enrollee, 65 years old, male no disability 0.295 – – – – Factor 1: Chronic diastolic HF, HCC 85 .0317 Factor 2: AKI with tubular necrosis, HCC 135 0.415 Factor 3: Disease interaction HCC 85 and renal 0.266 Risk score 0.295 0.317 0.415 0.266 Total risk score: 1.293 Enrollee, 66 years old, male, no disability 0.295 – – – Factor 1: Diabetes without complications, HCC 19 0.102 Factor 2: Heart failure, NOS, HCC 85 0.317 Factor 2: Alcoholic cardiomyopathy, HCC 85 Factor 3: Disease interaction DM*CHF 0.151 Risk score 0.295 0.102 0.317 0.151 Total risk score: 0.865
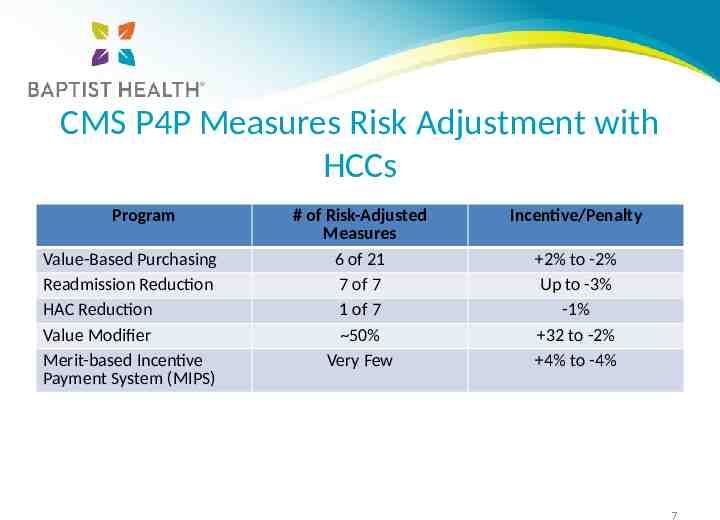
CMS P4P Measures Risk Adjustment with HCCs Program Value-Based Purchasing Readmission Reduction HAC Reduction Value Modifier Merit-based Incentive Payment System (MIPS) # of Risk-Adjusted Measures 6 of 21 7 of 7 1 of 7 50% Very Few Incentive/Penalty 2% to -2% Up to -3% -1% 32 to -2% 4% to -4% 7
Development of Process Education – Management team – Auditor/educators – CDI staff – Coding staff (task force meeting) – Physicians advisors Operating with limited budget – Staff – Education – Software for outpatient
Education On HCC Impact 8 hospital system – 350-400 employed physician practices Specialty groups – Hospitalist – Cardiology Peer-to-peer education Ancillary departments – Wound care nurses – Dieticians
Condition Categories CC 42% C HCC MCC 16% 10
TOP 5 BMI 19 or 40 and corresponding diagnosis CHF, acuity and specificity Malnutrition Diabetes associated complication or chronic condition(s) Primary and secondary cancers 11
TOP 5 We recognize the following: Most commonly known as “chronic” conditions 42% of HCC’s are also CC’s 16% of HCC’s are MCC’s These conditions also affect SOI/ROM for the in-patient encounter Affect the RAF scores for the calendar year Help provide an accurate description of patient care and utilization of resources Affect Quality programs MOST IMPORTANTLY WE ALREADY DO IT! 12
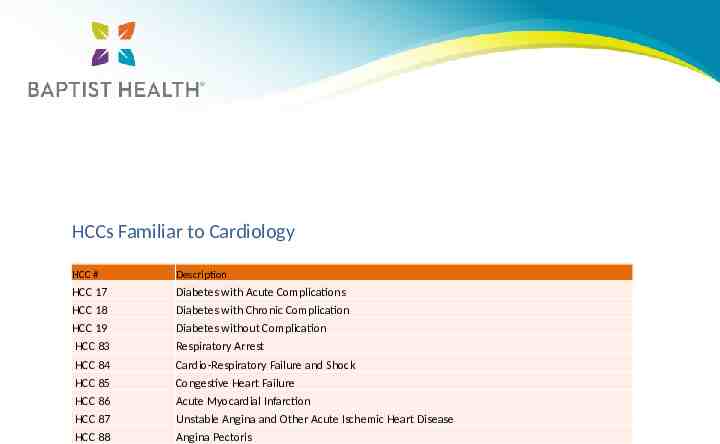
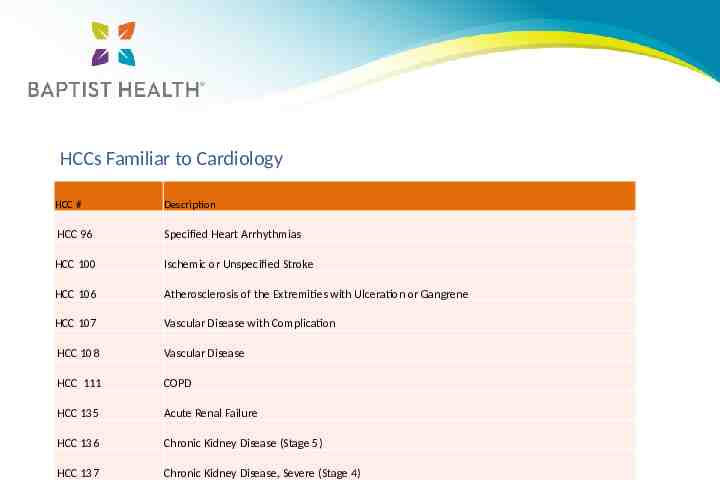
HCCs Familiar to Cardiology HCC # Description HCC 17 Diabetes with Acute Complications HCC 18 Diabetes with Chronic Complication HCC 19 Diabetes without Complication HCC 83 Respiratory Arrest HCC 84 Cardio-Respiratory Failure and Shock HCC 85 Congestive Heart Failure HCC 86 Acute Myocardial Infarction HCC 87 Unstable Angina and Other Acute Ischemic Heart Disease HCC 88 Angina Pectoris
HCCs Familiar to Cardiology HCC # Description HCC 96 Specified Heart Arrhythmias HCC 100 Ischemic or Unspecified Stroke HCC 106 Atherosclerosis of the Extremities with Ulceration or Gangrene HCC 107 Vascular Disease with Complication HCC 108 Vascular Disease HCC 111 COPD HCC 135 Acute Renal Failure HCC 136 Chronic Kidney Disease (Stage 5) HCC 137 Chronic Kidney Disease, Severe (Stage 4)
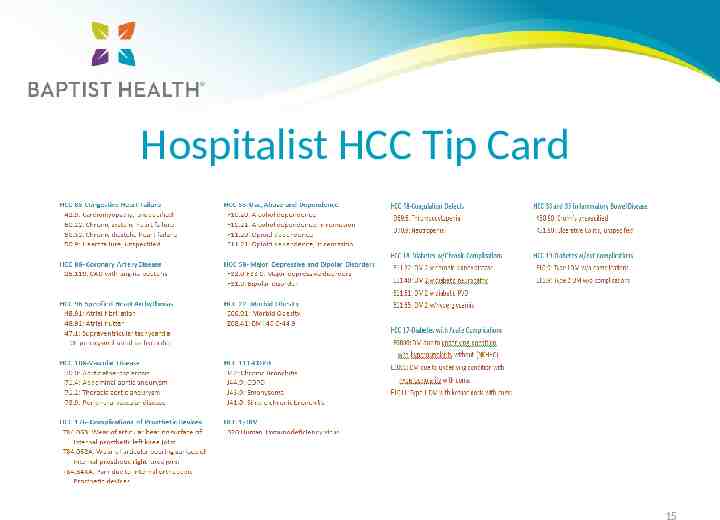
Hospitalist HCC Tip Card 15
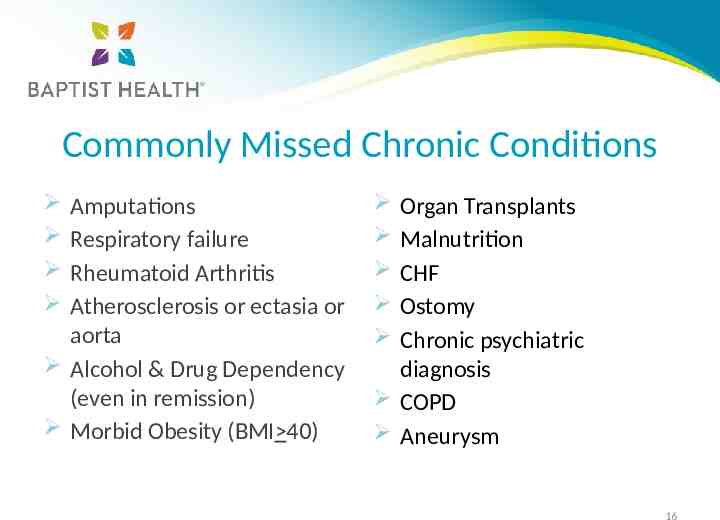
Commonly Missed Chronic Conditions Amputations Respiratory failure Rheumatoid Arthritis Atherosclerosis or ectasia or aorta Alcohol & Drug Dependency (even in remission) Morbid Obesity (BMI 40) Organ Transplants Malnutrition CHF Ostomy Chronic psychiatric diagnosis COPD Aneurysm 16
Re-admission Rates Don’t forget to document “Z codes” – Social determinants of health including: Non-compliance Substance abuse – Other “Z” codes Z51.5-Encounter for palliative care Z Z56*-Problems r/t employment and unemployment Z59*-Problems r/t housing and economic circumstances 17
ED Outpatient Strategy for developing a starting point Start small Meeting with key people to discuss – ED physician – ED manager – CDI staff – CDI Director/Manager/Coordinator – CDI Auditor/Educator – Case management – Quality 18
Identify Barriers CDI would distract from patient care Be in the way Lack of understanding of query process Lack of understanding of documentation to capture severity 19
CDI for Inpatient Admission from ER Benefits for Medical Necessity – Timely query for the most accurate principle diagnosis – Ensure the documentation is consistent from the ED to the admission – Accurate GLMLOS and status from the time of admission 20
Education One on one education with ED providers – Use our PA to help with education Education for ED staff – CDI staff provide education Start simple and gradually build on the education 21
Take-A-Ways HCC diagnoses directly affect capitated payments to a health plan for its Medicare Advantage members For providers, HCC diagnoses are used to risk-adjust quality and cost measures that can affect payment Remember HCCs, CCs and MCCs overlap which affect the RAF scores for the calendar year Implementing ED CDI program start small 22
Thank You [email protected] [email protected] 23