Radiology Resource Nurses Sheryl Redlin-Frazier, RN, MSN Jennifer















21 Slides1.72 MB
Radiology Resource Nurses Sheryl Redlin-Frazier, RN, MSN Jennifer Glenn, RN, MSN, CPN Rachel Hale, RN, DNP Brittany Justice, RN, MSN Ashley Vosilla, RN, MSN - Infographics
Objectives: Understand the history of the Radiology Resource Nurse (RRN) role Discuss current state of the RRN role Identify future goals of the RRN role
Novemb Need for Radiology Resource Nurse (RRN) identified er 2018 Decemb er 2018 March 2019 May 2019 Fall 2019 Initial RRN Job Description created Radiology Resource Nurse Role created Inpatient and Radiology Nursing & Technologist (IRNT) Taskforce created Barcode Medication Administration (BCMA) implemented Brittany Justice hired as Radiology Nursing Educator (August) Rachel Hale and Schuyler Jung-Figura hired as Clinical Staff Leaders of Radiology Nursing Revision of RRN Job Description Visual Notification System Trial CURRE Radiology Department specific education and SOP development NT HCAHPS/iRounding Ticket-to-Ride FUTURE Collaboration with VUH Float Pool
November 2018 Need for Nursing Coverage in Radiology Department identified by the State in response to a Sentinel Event
December 2018 The Radiology Resource Nurse (RRN) is a Registered Nurse that is critical care trained who acts as a clinical liaison between VUH patient care areas and the Department of Radiology. The RRN applies the nursing process to provide continuity of care while a patient is in the Department of Radiology for an imaging encounter. The RRN is responsible for collaborating with the Health Care Team through assessment and observation of/for: Potential instability or a change in condition; Maintain infection control measures; Contrast allergy response management per protocol; Assessment of intravenous access and complications such as infiltrations; Facilitate communication between Radiology staff, Radiologists, and Inpatient care teams; Assist with patient throughput; Intervenes in High Risk Events
The Radiology Resource Nurse does not: Take a patient assignment; Assume care of a patient while in the Radiology Department. Per the “Transport of Patients Receiving Medications That May Cause Impaired Consciousness or Undesired Changes in Vital Sign” Standard Operating Procedure, the RN/paramedic accompanies the patient when: o IV medication has been administered within the past 30 minutes for minimal sedation/anxiolysis in preparation for a procedure/test. Patient is monitored utilizing pulse oximeter during transport and until patient returns to baseline neurocognitive status, maintaining consistent level of care for patients while off the unit. o New IV analgesic or sedative medication (e.g., benzodiazepine, opioid) has been administered within the past 30 minutes. o Patient is on PCA/epidural/continuous controlled substance infusion with a change in medication, dose, concentration, or rate of administration within the last hour, maintaining consistency with a. MM SOP - Patient-Controlled Analgesia (PCA) and Continuous Controlled Substance Infusion: Administration and Management; and b. MM SOP - Epidural Analgesia Administration and Management. o Patient is receiving cardiac/telemetry monitoring. A RN/paramedic trained in basic arrhythmia accompanies the patient during transport and throughout the procedure/test unless it is confirmed that monitoring can be maintained by a qualified telemetry technician. o Patient needs observation based on the criteria above or RN/Paramedic judgement and there is not a RN/Paramedic to receive and observe the patient during testing or procedure. RN/Paramedic will document their assessment supporting their decision.
March 2019 24/7/365 coverage 7.2 FTEs o o 4 Day Shift RNs: 0645-1915 2 RNs Monday –Friday 1 RN Saturday-Sunday 4 Night Shift RNs: 1845-0715 2 RNs Monday –Friday 1 RN Saturday-Sunday Holidays 1 Day Shift RN 1 Night Shift RN
May 2019 The Inpatient and Radiology Nursing & Technologist (IRNT) Taskforce, comprised of nurses, techs, pharmacists, and respiratory therapists from Radiology, ICUs, and Acute Care areas, was created to: Focus on the provision of safe patient care and transition of care between inpatient units and the Department of Radiology; Understand, assess, and monitor data regarding patient safety and outcomes related to transition of care between inpatient units and the Department of Radiology o Objective data from Veritas reviews o Observational data from purposeful rounding o Nurse-patient experience o Rapid response data o Literature review Foster the development of a sustainable collaboration and culture of safety between inpatient care units and the Department of Radiology.
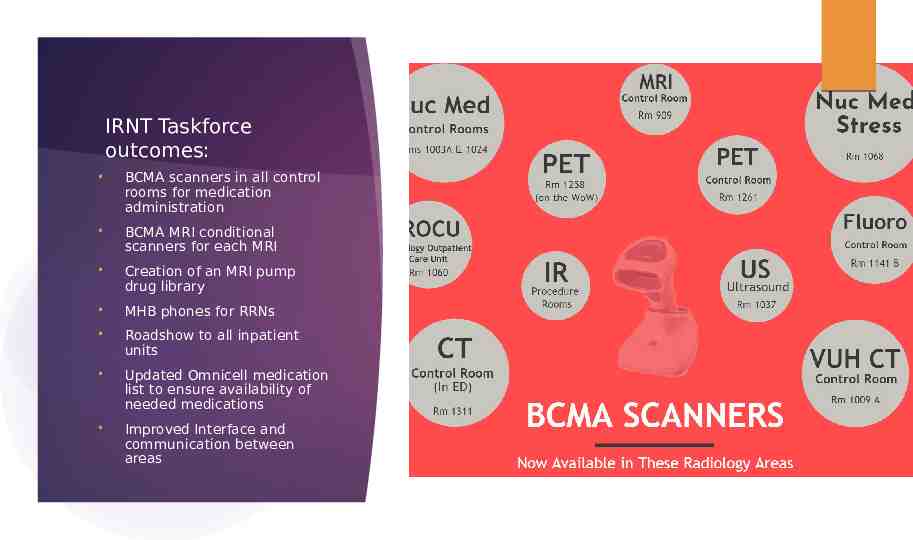
IRNT Taskforce outcomes: BCMA scanners in all control rooms for medication administration BCMA MRI conditional scanners for each MRI Creation of an MRI pump drug library MHB phones for RRNs Roadshow to all inpatient units Updated Omnicell medication list to ensure availability of needed medications Improved Interface and communication between areas
Fall 2019 Brittany Justice, RN, MSN is hired as the Nursing Education Specialist for Radiology, Noninvasive Cardiac Diagnostics, and Clinical Research Center. Rachel Hale, RN, DNP and Schuyler Jung-Figura, RN, BSN are hired as the first ever Clinical Staff Leaders in Radiology Nursing
CURRENT The RRN Job Description has been revised to include the following RRN interventions: Pacemaker monitoring: RRN will monitor patients with pacemaker/ICD during MRI scan, as outlined in the “Radiology SOP-Cardiac Implantable Electronic (CIED) in MRI” SOP; MRE: RRN will verify order and administer IM Glucagon as prescribed; Urogram: RRN will verify order and administer Lasix and Fluid Bolus as prescribed; Cystogram: RRN will assist with Foley Catheter insertion and management; COVID screening: RRN will assist with rapid pre-procedure COVID screening as outlined on the VUMC COVID website COVID notification: RRN will assist with clearing Radiology Halls prior to transport of COVID suspected/confirmed patient Nursing Skills: o PIV placement, management, and assessment o PICC/Central Line management and assessment, including accessing and de-accessing patient ports o Foley catheter insertion and management o Medication administration per order o Venipuncture
Cap the Line, Every Time Target Audience: CT and MRI technologists Visual Notification System Trial: Instructor: Sonia Duffey, RN 2-week trial How do lines become infected? Pre-survey: 55 responses Importance of using a swab cap Post-survey: 12 responses Prevention of CLABSI. Swab Cap use demonstration. Patient waiting for imaging and has been assessed by RRN. Patient imaging complete. Waiting for return to inpatient unit. Nuc Med patient: RN component complete, Patient waiting for additional imaging.
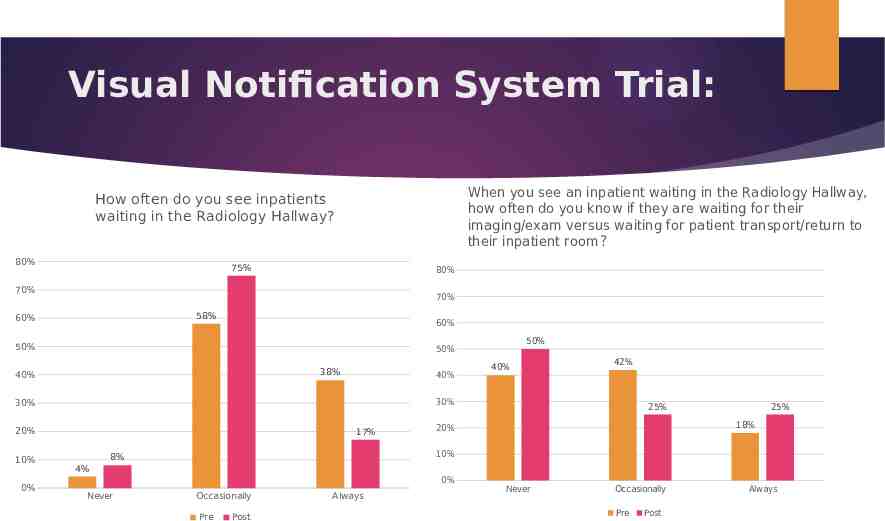
Visual Notification System Trial: When you see an inpatient waiting in the Radiology Hallway, how often do you know if they are waiting for their imaging/exam versus waiting for patient transport/return to their inpatient room? How often do you see inpatients waiting in the Radiology Hallway? 80% 75% 80% 70% 70% 58% 60% 60% 50% 38% 40% 40% 20% 0% 40% 42% 30% 30% 10% 50% 50% 17% 25% 25% 18% 20% 10% 8% 4% 0% Never Occasionally Pre Post Always Never Occasionally Pre Post Always
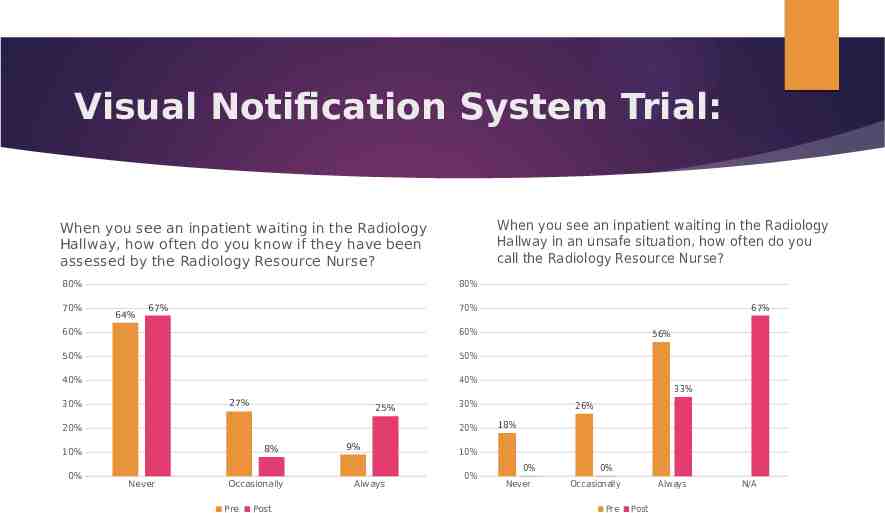
Visual Notification System Trial: When you see an inpatient waiting in the Radiology Hallway in an unsafe situation, how often do you call the Radiology Resource Nurse? When you see an inpatient waiting in the Radiology Hallway, how often do you know if they have been assessed by the Radiology Resource Nurse? 80% 70% 80% 64% 67% 60% 60% 50% 50% 40% 40% 27% 30% 25% 20% 8% Never Occasionally Pre Post 9% Always 56% 33% 30% 20% 10% 0% 67% 70% 26% 18% 10% 0% 0% Never 0% Occasionally Pre Always Post N/A
Visual Notification System Trial: When an inpatient is involved in a safety event in the Radiology Hallway, you can easily identify relevant patient information such as allergies, NPO status, diagnosis, medications, etc.? 80% 80% 64% 60% 53% 50% 50% 40% 40% 33% 18% 0% 20% 15% 9% 10% Occasionally Pre Always Post 13% 10% 9% 0% Never 44% 37% 30% 30% 20% 73% 70% 70% 60% In your opinion, how often do safey events occur involving inpatients waiting in the Radiology Hallway? N/A 9% 9% 6% 6% 9% 0% Never 1-2 times/ shift 2 or more times/shift Pre Post 1 time/week More than 1 time/week
What suggestions do you have for improving the care of inpatients waiting in the Radiology Hallway? Pre-Survey: A system in place to identify if the patient is coming or going from the department & it would be helpful to know where they are supposed to be going (CT/Ultrasound/Nuc Med/MRI) and coming from (which unit are they from) Round trip for patient transport needs to come back! It increases the risk for harm tremendously and I have personally seen it happen multiple times since they were told to not do a roundtrip. Modalities should label the patient as incoming or outgoing [stickers, hallway signs that can be flipped (one side incoming and one side outgoing) prior to placing the patient in the hallway. Or if a patient is waiting for a scan that will occur in an extended amount of time that patient should be labeled that way. It is my opinion that inpatients that are waiting in the hallways should be continuously monitored and not left alone SBAR handover document Round trip transport. we need more transporters, then patients wouldn't be waiting for long periods of time unattended. Easier access to a computer for the RRN to look up patients when they need care in the hallways Looking in to RRN phone lines that do not have "dead zones." Post-Survey: I work night shift where there is a pretty consistent system to identify our inpatient travels (coming or going). Our night RRN's are awesome at monitoring the flow of patients before this new visual system was instituted. During my night shift, the nurses are always available if we need them
What did we learn? There is a need for improved communication of inpatients in the Radiology department; There are concerns about patient safety in the Radiology Hallway; however, there are minimal safety events reported. Day shift and Night shift RRNs may have different visibility due to varying workload and demands. Limitations: Response rate: pre-survey: 55 vs post-survey: 12 Potential lack of awareness of study by various Radiology staff Inability to see post-it notes on stretchers: too small, didn’t stick to beds Competing priorities of RRNs: May not have been able to place a post-it on every stretcher Next Steps: Ticket-to-ride, SBAR Handover Evaluate Transport Staff Resources
FUTURE HCAHPS scores/iRounding: Rounding/Service Recovery on floors if a patient expresses a concern regarding their care/experience in the Radiology Department Ticket-to-Ride: SBAR handover to improve awareness and care of patients in Radiology Department Collaboration with the VUH Float Pool to help fill staffing vacancies USGPIV training for RRN staff How can we improve the care of your patients in the Radiology Department? What can we do better for you?
References: Standard Operating Procedure: Transport of Patients Receiving Medications That May Cause Impaired Consciousness or Undesired Changes in Vital Signs https://vanderbilt.policytech.com/dotNet/documents/?docid 16006