Screening, Brief Intervention, and Referral to Treatment (SBIRT)












29 Slides2.96 MB
Screening, Brief Intervention, and Referral to Treatment (SBIRT) Core Curriculum: Referral to Treatment The University of Iowa College of Nursing With funding from the Substance Abuse and Mental Health Services Administration (SAMHSA)
Goals for Today Identify factors that make primary care an ideal setting for SBIRT Identify options on the substance use care continuum Describe practical aspects of making successful treatment referrals Apply the SAMHSA Treatment Locator to your clinical location
Primary Care and SBIRT Primary care is one of the most opportune points of contact for substance use issues. Many patients are more likely to discuss this subject with their healthcare provider than with a family member, therapist, or rehab specialist.
Primary Care and SBIRT Given the prevalence of substance use disorder nationwide, it makes good sense for primary care practitioners – rather than trauma centers or specialists – to be a first line of response.
Primary Care and SBIRT As discussed earlier Approximately 5% of patients screened will require a referral to treatment Substance use disorder is a chronic and relapsing illness, so continuous monitoring is needed Monitoring and follow-up in primary care is essential
Primary Care and SBIRT Address the “treatment gap” Only 10% with substance use disorder (SUD) receive any kind of treatment Over 40% with SUD also have mental illness, but less than half (48%) get treatment for either Overcome barriers, stigma, misbeliefs Not a moral weakness or willful rejection of social norms Deserves same level of attention as other chronic health concerns
Reasons for Hope & Optimism Addiction to alcohol or drugs is a chronic but treatable brain disease that requires medical treatment, not moral judgment Evidence-based treatments – both medications and behavioral therapies – can save people’s lives and restore health, well-being, and function
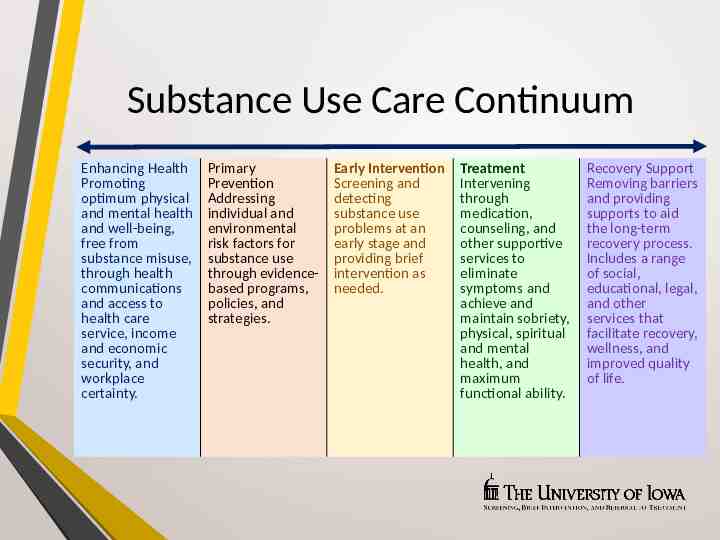
Substance Use Care Continuum Enhancing Health Promoting optimum physical and mental health and well-being, free from substance misuse, through health communications and access to health care service, income and economic security, and workplace certainty. Primary Prevention Addressing individual and environmental risk factors for substance use through evidencebased programs, policies, and strategies. Early Intervention Screening and detecting substance use problems at an early stage and providing brief intervention as needed. Treatment Intervening through medication, counseling, and other supportive services to eliminate symptoms and achieve and maintain sobriety, physical, spiritual and mental health, and maximum functional ability. Recovery Support Removing barriers and providing supports to aid the long-term recovery process. Includes a range of social, educational, legal, and other services that facilitate recovery, wellness, and improved quality of life.
Treatment Options Substance Use Disorder Treatment (like treatment for most other illnesses) is designed to Stop or reduce major symptoms (harmful misuse) Improve health and social function Recognize and manage risks for relapse Levels of care include Outpatient services Intensive outpatient/Partial hospitalization services Residential/Inpatient services Medically-managed Intensive Inpatient services
Treatment Options Counseling and other psychosocial rehabilitation services Medications Involvement with self-help (AA, NA, Al-Anon) Complementary wellness (diet, exercise, meditation) Combinations of the above
Treatment Options Level of care determined by illness severity Dependent or nondependent substance user? Medical or psychiatric comorbidities? Outpatient often successful Inpatient treatment Reserved for those with more serious illness
Guidelines for Greatest Success Determine if patient is drug or alcohol dependent and needs medical detoxification Nondependent substance abusers are usually treated as outpatients unless there are other risk factors Most patients can be successfully served in outpatient treatment
Strong Referrals When your patient is ready Make a plan with the person Actively participate in the referral process the warmer the referral handoff, the better the outcome!
Strong Referrals When your patient is ready Decide how you will interact/communicate with the treatment provider Confirm your follow-up plan with the person Decide on ongoing follow-up support strategies you will use
Strong Referrals The “warm-handoff referral” The clinician directly introduces the patient to the treatment provider Purpose is to establish an initial direct contact between the patient and the treatment counselor Confers existing trust and rapport Dramatically increases success compared to passive referrals
Plan for the Nuts and Bolts Whom do you call? Do you have access to referral resource information? What form do you fill out? What support staff can help?
Choosing a Treatment Provider Language ability/cultural competence Family support Services that meet the patient’s needs Record of keeping primary care provider informed of patient’s progress and ongoing needs Accessible location/transportation
Payment for Services Does the provider accept your patient’s insurance? Will the patient need to get prior insurance authorization? If the patient does not have insurance, does the provider offer services on a sliding-fee scale?
What Should You Expect? Substance use treatment services should provide you ongoing updates with a valid release of information If they do not, you may choose to refer elsewhere (if options exist!) Work to cultivate partnerships
What Should You Expect? Substance use treatment facilities should provide you with a structured discharge plan discussing Ongoing treatment needs Recovery needs Sources of assistance Recommended providers
What Should You Expect? Programs change over time Maintain an up-to-date roster Public and private treatment Self-help resources in your community
Common Mistakes to Avoid Rushing into “action” and making a treatment referral when the patient isn’t interested or ready Referring to a program that is full or does not take the patient’s insurance Not knowing your referral base Not considering pharmacotherapy in support of treatment and recovery Seeing the patient as “resistant” or “self-sabotaging” instead of having a chronic disease
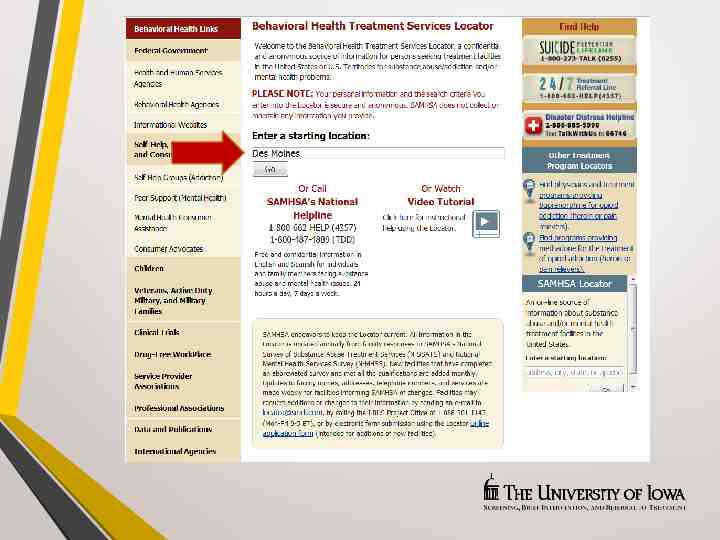
Referral Resources SAMHSA’s National Treatment Facility Locator http://findtreatment.samhsa.gov
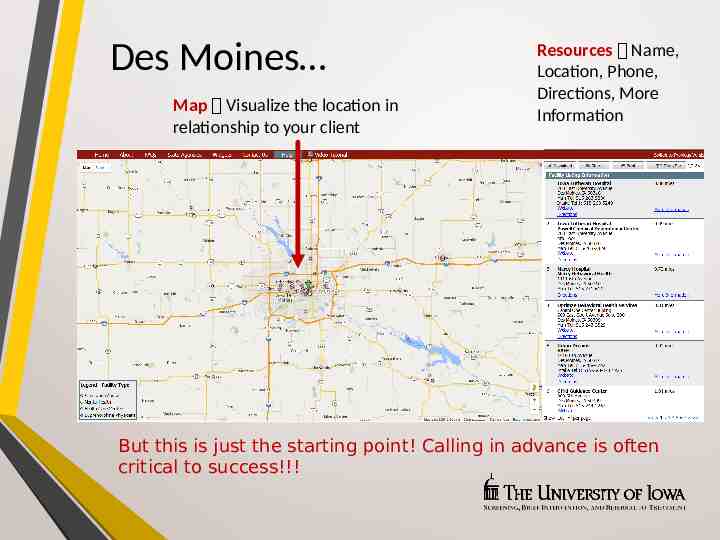
Des Moines Map Visualize the location in relationship to your client Resources Name, Location, Phone, Directions, More Information But this is just the starting point! Calling in advance is often critical to success!!!
Back to the SBIRT Process Statistically speaking Many prescreens are negative; few full screens needed Even with full screen, many are low risk Being READY is the key! Brief intervention Feeling comfortable following the guide/having the conversation Referral to treatment Knowing who/where/what is available; warm handoff
Summary Treatment works With a minimal amount of preparation, you can know what is available in your community Clarify your procedures for referral Warm handoffs work best Follow up!
Acknowledgements Content in this educational module was provided by the Substance Abuse and Mental Health Services Administration (SAMHSA) under grant to the University of Iowa with permission to adapt and use in training. Grant #1H79TI025939-01
Acknowledgements