OVERVIEW OF ARIZONA MEDICAID SERVICES, DUE PROCESS RIGHTS, AND






69 Slides852.24 KB
OVERVIEW OF ARIZONA MEDICAID SERVICES, DUE PROCESS RIGHTS, AND THE CHANGING LANDSCAPE OF AHCCCS Presenter: Sarah E. Kader Staff Attorney Arizona Center for Disability Law
Outline of Training 1. Overview of Medicaid & AHCCCS 2. Update on Medicaid Expansion 3. Affordable Care Act Overview 4. Questions
Arizona Center for Disability Law Non-profit public interest law firm AND Protection and Advocacy (P&A) agency for Arizona Part of network of agencies ‒ one in every state and territory ‒ providing protection to people with disabilities through legally based advocacy Funded primarily through federal grants Dedicated to protecting the rights of individuals with physical, mental, psychiatric, sensory and cognitive disabilities
Types of Services Provided by the Center Information and advice regarding legal rights Representation of individuals in negotiations, administrative proceedings, and court Impact litigation to remedy systemic problems Investigation of abuse and neglect allegations Outreach and training on legal rights and selfadvocacy Technical assistance to groups and individuals on disability-related legal issues Advocacy for policy and legal reforms that benefit people with disabilities
OVERVIEW OF MEDICAID
Medicaid A joint federal and state program that provides health care for people with low incomes and limited resources Enacted in 1965 as part of President Johnson’s War on Poverty Consists of acute care services, long term care services, and behavioral health services Medicaid Act Title 19 of Social Security Act, 42 U.S.C. 1396-1396v
Who Does Medicaid Serve? Largest public health insurer covers 1 in 10 Americans As of June 2011: 52.6 million enrolled 13.9 million aged and disabled enrolled 233,000 aged and disabled enrolled in Arizona Kaiser Commission on Medicaid Facts: http://www.kff.org/medicaid/upload/8050-05.pdf
MEDICAID FRAMEWORK AND PRINCIPLES
Medicaid Act Principles Statewide Medical Necessity (but no federal definition) Not experimental Open-ended federal funding of necessary services Amount, duration, and scope – sufficient to achieve purpose No discrimination based on condition
Medicaid Act Principles Comparability of services between and within eligibility groups Reasonable promptness (i.e. no waiting lists) Freedom of Choice of Provider (but providers not mandated to participate) – does not apply in AZ Equal Access to Services - enlist enough providers so that services are broadly available Due Process Guarantees
Medicaid Eligibility- 4 Requirements Limited income/resources Citizenship or proper immigration status State residency Must fit into category of eligibility Mandatory and Optional categories
MEDICAID SERVICES
Mandatory Medicaid Services 42 U.S.C. §1396d Inpatient and outpatient hospital services Physician services Laboratory and x-ray services Home health services for individuals entitled to receive nursing facility services Early and Periodic Screening, Diagnosis, and Treatment Services (EPSDT)
EPSDT Services 42 U.S.C. §1396d(r) Mandatory service for children and youth under 21 Established by Congress in 1967 with intent to be the “nation’s largest preventative health program for children,” amended in 1989 to broaden scope of services Intended to be a comprehensive package of screening, diagnostic, and treatment services
EPSDT Services All necessary health care to “correct or ameliorate” physical or mental problems or conditions 42 U.S.C. 1396d(a) Covers all medically necessary services, even if service is not in the state plan and/or is not provided to adults
Optional Medicaid Services 42 U.S.C. §1396d Clinic services Private duty nursing services Prescription drugs Physical, occupational, speech, hearing, and language therapy Home health services for individuals not eligible for nursing facility services
MEDICAID IN ARIZONA
Medicaid in Arizona The Basics Arizona Health Care Cost Containment System (AHCCCS; pronounced “Access”) ‒ single state Medicaid agency. Entire AHCCCS program run as statewide managed care system; most states are fee-forservice. Arizona has a Section 1115 Waiver from the federal government (CMS) which exempts it from key requirements of the Social Security Act (Medicaid Act).
ALTCS: Long Term Care Delivery System Arizona Long Term Care System (ALTCS) ‒ pronounced “Alltecs”. Serves two populations: Elderly and Physically Disabled (EPD), and Developmentally Disabled (DD). Eight health care plans provide long term care ‒ DDD is one of them. ALTCS members get behavioral health and acute care services from ALTCS health plan.
DDD Rule Exceptions Acute Care Services DDD/ALTCS members are assigned to an AHCCCS acute health plan. Behavioral Health Services DDD/ALTCS members receive behavioral health services from RBHA system.
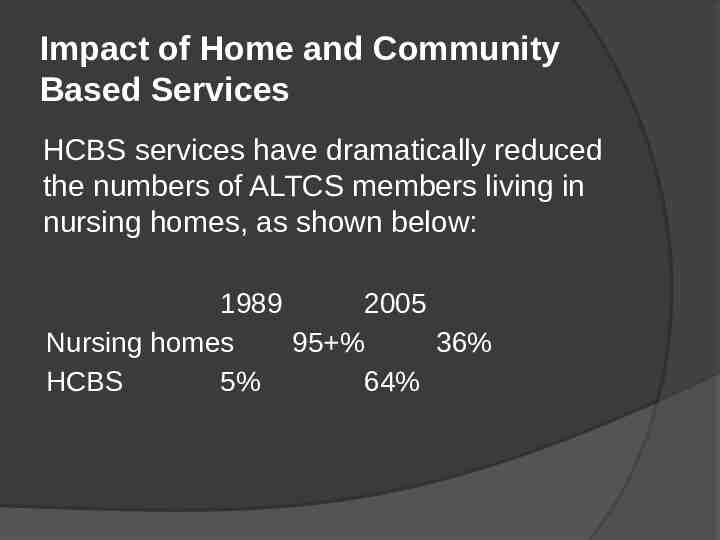
Impact of Home and Community Based Services HCBS services have dramatically reduced the numbers of ALTCS members living in nursing homes, as shown below: 1989 2005 Nursing homes 95 % 36% HCBS 5% 64%
AHCCCS CostContainment Lowest pharmacy rates in country. Third in the nation for lowest cost per Medicaid enrollee. Arizona spends 3,035 per member per year, 976 less than the national average.
AHCCCS/ALTCS Eligibility Generally No disability requirements for acute care AHCCCS. ALTCS has financial and disability requirements: Must be at risk of institutionalization. Pre-Admission Screening Test (PAS) measures risk of institutionalization. EPD PAS A.A.C. R9-28-304 DD PAS A.A.C. R9-28-305
AHCCCS Enrollment AHCCCS provides Medicaid services to more than 1 million Arizonans. Serves 18% of Arizona population. 11% of AHCCCS population is Native American.
GETTING SERVICES FROM AHCCCS AND ALTCS
AHCCCS Coverage Requirements For AHCCCS/ALTCS to cover a service, it must be: A covered service Medically necessary Cost-effective Non-Experimental Federally reimbursable (i.e. can get FFP) A.A.C. R9-22-201(B)
AHCCCS Acute Care Covered Services Physician services Prescription drugs Hospital Services Transportation to medical services Physical, occupational, speech therapies Durable medical equipment and supplies EPSDT services Behavioral health services Emergency care Pregnancy care Dialysis X-Rays Lab work Surgery Organ Transplants
ALTCS Covered Services All AHCCCS acute care services Behavioral health services EPSDT services Nursing home services ICF/MR (intermediate care facility for the mentally retarded)
ALTCS HCBS Services Case management Speech, physical, and occupational therapies Personal care Attendant care Respite Habilitation Home modifications Medical equipment & supplies Emergency alert system Transportation Home delivered meals DD day care Assisted living facilities Home health Aid and Nurse
Medically Necessary No federal definition of medically necessary “Medically necessary” means a covered service provided by a physician or other licensed practitioner of the healing arts within the scope of practice under state law to prevent disease, disability, or other adverse health condition or their progression, or to prolong life.” Arizona Definition: A.A.C. R9-22-101(B)
Cost-Effective Arizona does not define “cost-effective” in statute, regulation or policy. For ALTCS members: Generally argue that services under the cost of institutionalized care are cost-effective. Use Cost-Effectiveness Study – measures cost of nursing home case against cost of services in the community.
Non-Experimental For a service to be non-experimental, it must be associated with treatment or diagnostic evaluation and: Generally and widely accepted as a standard of care in the practice of medicine in the United States; OR Peer-reviewed articles in medical journals published in the United States that support the safety and effectiveness of the service; OR If no articles, and for a rare, novel or relatively unknown service, the weight of opinions from specialists who provide the service and attest to the safety and effectiveness of the service. A.A.C. R9-22-101(B)
Standard of Care Means a medical procedure or process that is accepted as treatment for a specific illness, or injury, medical condition through custom, peer review, or consensus by the professional medical community. A.A.C. R9-22-101(B)
MEDICAID DUE PROCESS REQUIREMENTS
Due Process Guarantees Right to Medicaid due process protected by the Due Process Clause of Constitution Holding that when welfare benefits may be terminated, beneficiary has due process rights to an effective notice and pretermination hearing. Goldberg v. Kelly, 397 U.S. 254, 266 (1970)
Medicaid Due Process Rights Written File notice of denial/termination/reduction appeal, even without written notice Expedited Fair decision hearing Representation at hearing Review evidence prior to hearing and get copies Present evidence and cross examine witnesses Continuation of existing services pending hearing; liable for costs, if you lose Timely, written decision ‒ within 90 days of appeal Reimbursement for costs if services pending appeal if wrongly denied
AHCCCS ADMINISTRATIVE APPEALS AND HEARINGS PROCESS
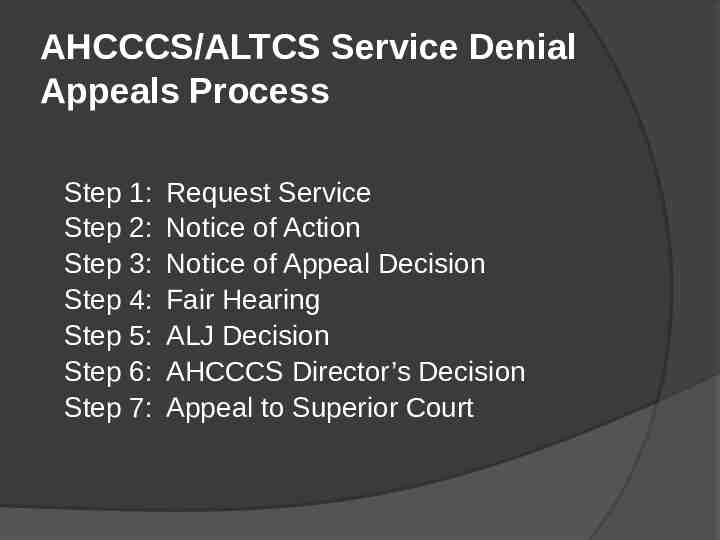
AHCCCS/ALTCS Service Denial Appeals Process Step 1: Step 2: Step 3: Step 4: Step 5: Step 6: Step 7: Request Service Notice of Action Notice of Appeal Decision Fair Hearing ALJ Decision AHCCCS Director’s Decision Appeal to Superior Court
Requesting a Service: Letter of Medical Necessity Key to effectively requesting AHCCCS services. Letter from member’s doctor or specialist that outlines reasons why member needs service. When requesting LMN, include: signed release, and “How to Write Effective Letter of Medical Necessity”‒ general statements that member “will benefit” or that doctor “supports” treatment are not enough.
Notice of Action (NOA) Must be issued within 14 days of service request. Failure to provide NOA within timeframe constitutes a denial. Time frame may be extended by 14 days. NOA Contents: Legal and factual reasons for denial, termination or reduction Where to file appeal
Right to Continuation of Services Filing deadline: 10 days from NOA Must involve termination, suspension, or reduction of current services. Original authorization period has not expired. If beneficiary loses, liable for cost of services. A.A.C. R9-34-224
Practice Tip: Requesting an Appeal Filing Deadlines: 60 days after Notice of Action, OR 10 days after NOA to request continuing services; Can be filed even if NOA not issued. Appeal letter can request the following: Expedited resolution of appeal Continuing services pending appeal Copy of health plan file Right to give additional info to plan
Notice of Appeal Resolution Issued by health plan within 30 days of letter of appeal 14 day extension available Must: Advise member how to request fair hearing. Provide legal and factual reasons for decision.
Right to Expedited Appeal Resolution Beneficiary or physician requests after Notice of Action Standard: “taking the time for standard resolution could seriously jeopardize the enrollee’s life or health, or ability to attain, maintain, or regain maximum function” Must resolve within three working days A.A.C. R9-34-214 and 215
Practice Tip: Requesting Fair Hearing Filing Deadline: 30 days from date of Notice of Appeal Resolution Letter should include: Request for hearing; Statement of issue(s) for hearing, including due process concerns; Request for copy of appeal file; Signed release and designation of representative; and Restatement of any request for continuing services, expedited hearing, or reimbursement.
Right to Expedited Hearing Beneficiary or physician requests after Notice of Expedited Appeal Resolution. AHCCCS Director makes decision three working days after receiving ALJ recommended decision. A.A.C. R9-34-219 and 220
THE FAIR HEARING Office of Administrative Hearings
Office of Administrative Hearings (OAH) Independent agency that conducts AHCCCS and ALTCS fair hearings. Hearing conducted by Administrative Law Judge (ALJ). OAH offices in Tucson and Phoenix.
Medicaid Beneficiary’s Right to Attend Hearing Beneficiary has right to attend hearing in person or by phone. If beneficiary does not have transportation and wants to attend in person, health plan must provide transportation to hearing. 42 CFR 431.250(f)(1) Send request letter to health plan and copy OAH and AHCCCS.
Standard & Burden of Proof Standard of Proof Preponderance of the evidence – used in civil cases. More likely to be true than not true. Burden of Proof Generally on the Complainant; HOWEVER, if health plan terminated or reduced existing service, should argue that plan should have burden of showing that Complainant had change in health condition that justifies change in services (case law from other states).
Practice Tip: Evidentiary Issues Rules of Evidence do not apply. All relevant evidence is admissible (A.R.S. 41-1092.07(D) & (F)(1)) Some ALJ’s give more weight to in-person testimony versus letters/declarations; HOWEVER, should argue that in-person testimony of non-treating doctor should not be entitled to more weight than opinion of treating doctor provided via letter or declaration.
Practice Tip: Good Evidence re: Medical Necessity Testimony, letter, or declaration of: treating doctors/health professional. Examining doctors/health professional. client/parent ‒ person with knowledge of needs of person with disability. OPTIONAL: Documents used in experimental cases.
Practice Tip: Good Evidence re: Experimental Declaration/testimony from: treating doctor (should address medical necessity too) National experts ‒ medical school profs Medical journal articles Treatment guidelines/standard of care protocols from national organizations FDA guidelines Other health insurance coverage policies Medicare Private health insurance
Practice Tip: Conducting the Fair Hearing All OAH hearings are digitally recorded. Exhibits: Exchange of exhibits not required until hearing. Provide exhibit list and pre-label exhibits. If telephonic testimony ‒ have phone numbers. Can request post-hearing briefing: Raise deference to treating provider. Request payment for services pending appeal.
The Administrative Decisions ALJ Recommended Decision: Findings of Fact and Conclusions of Law. Issued to AHCCCS within 20 days of the close of the record, either after hearing or after briefing. OAH does not send copy to Complainant. Complainant may request copy for .25 per page. AHCCCS Director Decision: Issued 30 days after ALJ Decision. Director may accept, reject, or modify decision.
Motion for Reconsideration and/or Rehearing Filing Deadline: 30 days after service Basis for Reconsideration/Rehearing: Procedural irregularities or misconduct by party, witness, or OAH; Good reason for non-appearance; Newly discovered evidence; Decision result of passion/prejudice; or Decision not justified by evidence or law. Open Question ‒ Whether health plan can file for reconsideration/re-hearing.
Motion for Reconsideration and/or Rehearing Stays timeframes for filing Complaint for Judicial Review in Superior Court. Not required to exhaust administrative remedies. Health plan has right to file response. Director must issue final decision within: 15 days after response. If no response filed, five days after response period.
JUDICIAL REVIEW OF ADMINISTRATIVE DECISION
Overview of Appeal to Superior Court Pursuant to A.R.S. §12-901 et seq. Can Request De Novo Hearing ‒ 30 days from Complaint. Can Submit Additional Evidence ‒ before opening brief. Can get attorneys’ fees and costs.
Standard of Review The court shall affirm the agency action unless after reviewing the administrative record . . ., the court concludes that the action is not supported by substantial evidence, is contrary to law, is arbitrary and capricious, or is an abuse of discretion. Section 12-910(E)
Complaint for Judicial Review Filing Deadline: 35 days from date of Final Director’s Decision. Defendants are now health plan, AHCCCS, and AHCCCS Director. Venue: in county where beneficiary lives OR county where appeal held. A.R.S. 12-905(B) Civil filing fees apply; waiver possible. Regular service rules apply; AHCCCS will accept, but you may want to consider regular service to avoid delaying answer.
CURRENT STATE OF AFFAIRS
Medicaid Expansion Under the Affordable Care Act, Arizona had the opportunity to expand the Arizona Health Care Cost Containment System (AHCCCS), our Medicaid program, to thousands of uninsured, low-income residents. Arizona expanded Medicaid and so: all low-income individuals and families earning less than 138% of the federal poverty level (FPL) will be eligible for health insurance coverage through Medicaid. That includes individuals who make less than 15,000 per year; families of two who make less than 21,000 per year; and families of four who make less than 32,000 per year.
Medicaid Expansion We will get health coverage for over 25% more people. Approximately, 300,000 additional persons will have health care coverage as a result of the expansion. Approximately 225,000 adults without minor children in the home with incomes up to 100% of the federal poverty level will be covered because the freeze on enrollment for childless adults will end and another 65,000 adults (parents and childless adults) with incomes between 100-138% of the federal poverty level will be added to the AHCCCS program.
Medicaid Expansion Because Arizona expanded its AHCCCS program, the federal government will pay Arizona a higher reimbursement rate for childless adults costs. The health care costs for childless adults up to 100% of poverty will cost the state 702 million over 4 years (2013-2016) and the federal government will pay almost 4.8 billion for the coverage. http://www.azahcccs.gov/shared/Downloads/News/aca ahccc s costsummary.pdf. For adults between 100-138% of poverty, for the first 3 years, there are no costs to the state because the federal government will reimburse the state 100% of the health care costs. In the fourth year the reimbursement rate will be 95%. The federal government is expected pay Arizona over 1.4 billion for these health care costs.
Current State of Affairs Remember that the National and Local debates and changes are both important because Medicaid is a joint federal and state program. In regard to certain actions, what our State can do depends on what the Federal Government approves.
What You Can Do Write your Federal and State Legislators asking them to maintain Medicaid funding. Vote in local and national elections – make sure the people you vote for will fund the programs you care about. Don’t lose your current AHCCCS coverage, stay up to date with AHCCCS requests. Check mailings from your providers/AHCCCS. Check AHCCCS website for updates. Call ACDL if you are negatively affected by changes to AHCCCS eligibility.
AFFORDABLE CARE ACT Due process rights under the ACA, too Different process but somewhat similar Difference – if you appeal through your health plan and disagree with decision, there is an external review process. You can also file a complaint with the Office of Civil Rights here: http://www.hhs.gov/ocr/civilrights/compla int 68
THANK YOU! 69