MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Role of the


















36 Slides254.72 KB
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Role of the Pharmacist in the Care of Persons Living with Dementia MODULE 15 U.S. Department of Health and Human Services Health Resources and Services Administration January 2019 The U.S. Department of Health and Human Services, Health Resources and Services Administration developed this module under a contract. Some of the views expressed in this presentation module are solely the opinions of the author(s) and do not necessarily reflect the official policies of the U.S. Department of Health and Human Services or the Health Resources and Services Administration, nor does mention of the department or agency names imply endorsement by the U.S. Government.
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Copyright Language We purchased the images for Modules 1-12 from iStock by Getty. We accessed the images for Modules 13-16 using Google Find Free-to-Use Images. 2
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 3
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Learning Objectives After reviewing this module, the learner will be able to: Discuss the role of the pharmacist in identifying persons who should be evaluated for a diagnosis of dementia Explain the role of the pharmacist in choosing the appropriate medications for the treatment of Alzheimer’s disease and associated comorbidities (conditions that exist concurrently) Describe how pharmacists can monitor persons for problems such as medication failure, non-adherence and side effects, and the ways that intervention may occur Discuss the role of the pharmacist in caring for the person with advancing dementia Describe how the pharmacist can assist individuals who are caring for persons living with dementia 4
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Key Take-Home Messages Pharmacists have: Frequent contact with persons with dementia as well as their caregivers, which puts them in a position to address medication and disease-related concerns. Expertise to address issues related to medications used for dementia, as well as concomitant diagnoses. Knowledge to address co-morbid conditions treated with prescription and non-prescription medications. Resources and can offer education to persons and care partners regarding dementia treatment approaches as well as realistic expectations 5
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 2 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 6
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Identification of Persons Living with Dementia Pharmacists are likely to see both persons living with dementia and care partners on a regular basis. o They may be the first healthcare practitioner to recognize changes in behavior, memory and mood. o They can monitor for changes in persons with known pre-disposing conditions. o They may administer simple screening tests. o They may suggest referral to a diagnostician when appropriate. (Diagnosis of Alzheimer’s Disease and Dementia, 2016; Tett et al., 1993; Marasco et al., 2002; Neugroschl & Wang, 2011; The Montreal Cognitive Assessment, 2016) 7
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Conditions Associated with an Increase in Alzheimer’s Disease Occurrence Advanced age Atherosclerosis (deposits of fatty material in the arteries) Down Syndrome Family history Head injury Hypercholesterolemia (elevated cholesterol levels) Hyperglycemia/Diabetes Mellitus (high blood sugar) Hypertension (high blood pressure) (What We Know Today About Alzheimer’s Disease, 2016; Alzheimer’s Disease Genetics Fact Sheet, 2016; McGuinness et al., 2009; Alzheimer’s Research on Causes and Risk Factors, 2016; Alzheimer’s Disease, 2014; Kroner,2009) 8
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Common Initial Symptoms of Alzheimer’s Disease Pharmacists should consider further inquiry if any of the following are noted: o Memory loss or difficulty recalling the names of everyday objects (anomia) o Difficulty with performance of familiar tasks (apraxia) o Speech difficulty or difficulty understanding words (aphasia) o Inability to process sensory information (agnosia) o Decreased judgment o Difficulty with abstract thinking o Disorientation to time or place o Misplacing items o Loss of motivation o New “late onset” seizures and/or gait dysfunction in adults with Down syndrome (Diagnosis of Alzheimer’s Disease and Dementia, 2016; Mild Cognitive Impairment, 2016; Alzheimer’s Disease: Unraveling the Mystery, 2008; Neugroschl & Wang, 2009) 9
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Medication Review to Rule Out Drug-Induced Symptoms Some medications may cause side effects that mimic the early signs of dementia: o Anticholinergics Antihistamines Skeletal muscle relaxants Tricyclic antidepressants o Psychoactive agents Antipsychotics Benzodiazepines o High doses of corticosteroids o H2-receptor antagonists o Sedative hypnotics (Larson et al., 1984; Neugroschl & Wang, 2011; Radcliff et al., 2015; Allgaier & Allgaier, 2013; Lieberman, 2004; Ciriaco et al., 2013; Cantú & Korek, 1991) 10
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Case Study Part 1 HB is a 72-year-old female who has been a customer of her pharmacy for several years. She has been on lisinopril for her hypertension for several years, and has been an adherent person, typically refilling her medication 3-5 days before she is due to run out. Today she arrives to pick up her prescription nearly 2 weeks early. She hands the technician her new insurance card, and he takes it to the computer station to enter the information. Upon realizing that it is too early to fill HB’s prescription, the technician approaches the pharmacist. As the pharmacist approaches HB to explain that they can’t put the prescription through insurance at this time, she notices that HB is searching her wallet. HB tells the pharmacist, “I know I have a new insurance card, but I can’t seem to find it.” The pharmacist reminds HB that she has already provided the technician with her new card. HB shakes her head and laughs about how “scatterbrained” she has been over the last couple months. The pharmacist asks HB about her memory, and is told that it has been getting worse, and HB proceeds to provide a couple anecdotes about times when she has forgotten something that she normally found easy to remember. The pharmacist asks HB if she would be willing to take a short test to see if her memory issues might require a visit to a physician, and HB states that she would. 11
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 3 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 12
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Participation in the Drug Utilization Process for Alzheimer’s Disease Treatment Pharmacists should work with prescribers to ensure medications and doses are appropriate over the course of the disease. Mild-moderate Alzheimer’s disease o Cholinesterase Inhibitors Donepezil Galantamine Rivastigmine Moderate-severe Alzheimer’s disease o Cholinesterase Inhibitors Donepezil o N-methyl D-aspartate (NMDA) Receptor Antagonist Memantine 13
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Monitoring Initiation and Titration of Medications Pharmacists should make sure that medications are initiated at the correct dose, and titrated according to guidelines. o Minimize adverse events. o Ensure persons reach the optimum therapeutic dose. o Assess persons for hepatic disease or impaired renal function and contact prescribers for dose adjustments or medication substitution when necessary. (DeSimone & Viereck, 2011; Versijpt, 2014; Livingston & Katona, 2004; Farlow et al., 2010; Donepezil package insert, 2015; Rivastigmine package insert, 2015; Galantamine package insert, 2015; Memantine package insert, 2013) 14
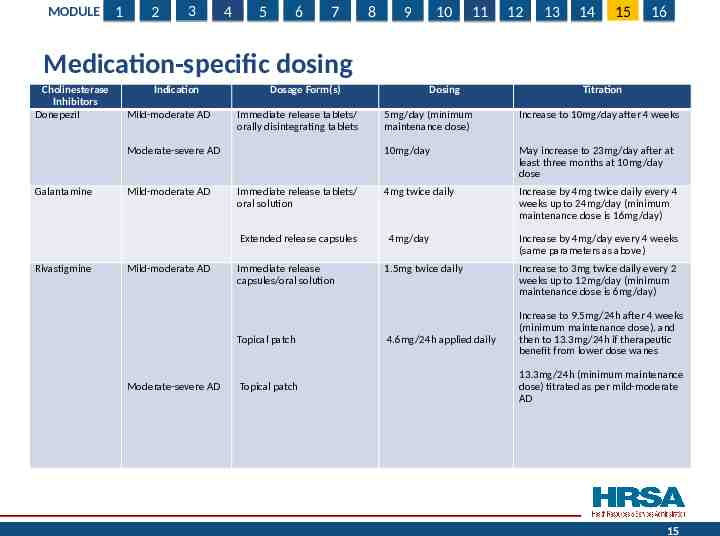
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Medication-specific dosing Cholinesterase Inhibitors Donepezil Indication Mild-moderate AD Dosage Form(s) Immediate release tablets/ orally disintegrating tablets Moderate-severe AD Galantamine Mild-moderate AD Immediate release tablets/ oral solution Extended release capsules Rivastigmine Mild-moderate AD Immediate release capsules/oral solution Topical patch Moderate-severe AD Topical patch Dosing Titration 5mg/day (minimum maintenance dose) Increase to 10mg/day after 4 weeks 10mg/day May increase to 23mg/day after at least three months at 10mg/day dose 4mg twice daily Increase by 4mg twice daily every 4 weeks up to 24mg/day (minimum maintenance dose is 16mg/day) 4mg/day 1.5mg twice daily 4.6mg/24h applied daily Increase by 4mg/day every 4 weeks (same parameters as above) Increase to 3mg twice daily every 2 weeks up to 12mg/day (minimum maintenance dose is 6mg/day) Increase to 9.5mg/24h after 4 weeks (minimum maintenance dose), and then to 13.3mg/24h if therapeutic benefit from lower dose wanes 13.3mg/24h (minimum maintenance dose) titrated as per mild-moderate AD 15
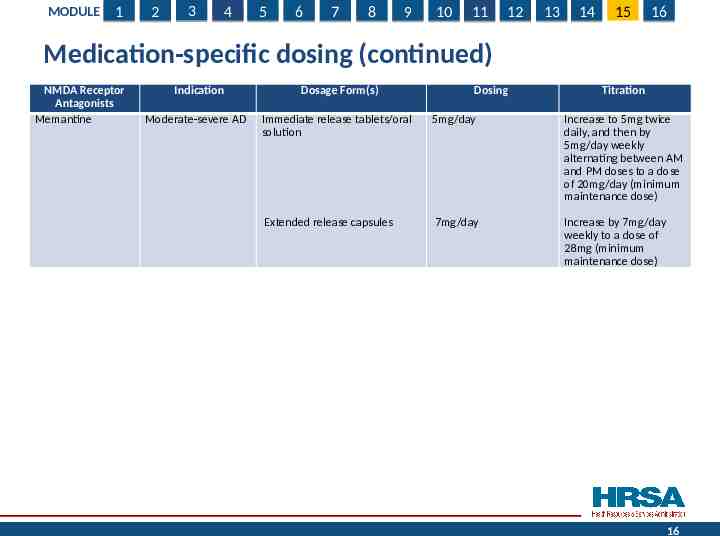
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Medication-specific dosing (continued) NMDA Receptor Antagonists Memantine Indication Dosage Form(s) Dosing Titration Moderate-severe AD Immediate release tablets/oral solution 5mg/day Increase to 5mg twice daily, and then by 5mg/day weekly alternating between AM and PM doses to a dose of 20mg/day (minimum maintenance dose) Extended release capsules 7mg/day Increase by 7mg/day weekly to a dose of 28mg (minimum maintenance dose) 16
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Educating the Person, Family and Care Partners Set realistic expectations with regard to drug therapy o Currently there is no cure. o Progression will continue, but advancement may slow. o Emphasize the need for adherence regardless of perception of benefit. o Explain what side effects may be seen with drug therapy, and provide strategies for addressing them. o Explain that symptoms and behaviors associated with Alzheimer’s disease may require changes or adjustments in drug treatments. o Advise that no over-the-counter (OTC) or nutraceutical medications should be started without the advice of the pharmacist or physician. Provide information about lack of regulation and efficacy data of nurtriceutical products. 17
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Educating the Person, Family and Care Partners (continued) Pharmacists should familiarize themselves with local resources for person and care partner education. o Keep a list of support groups in the area. o Appreciate that care partners of adults with Down syndrome and other types of intellectual disability may be parents, other kin, or community support agency staff. o Provide internet support sites. Be cognizant of how “tech-savvy” older adults might be. Caution about less reputable information. o Keep general information about dementia in the pharmacy to hand out as necessary. Make sure level of information is appropriate for degree of health-literacy. Consider using pictograms. Make sure font size, coloring, etc. are appropriate. 18
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Case Study Part 2 HB is diagnosed with Alzheimer’s disease. She receives a prescription for rivastigmine, 1.5mg by mouth twice daily, and her son picks the prescription up. A week and a half later, HB arrives at the pharmacy to pick up her lisinopril prescription for her hypertension. The pharmacist asks how she is doing taking the rivastigmine. HB states that it causes such frequent nausea, that she has stopped taking it, and plans to make an appointment with her physician to discuss other options, but has not yet done so. The pharmacist reminds HB that it is important for her to be on medication to slow the progression of Alzheimer’s disease since any loss of cognitive function while off medication may not be recoverable. Upon questioning, the pharmacist finds that HB was taking her medications on an empty stomach. It is suggested that HB re-initiate therapy, and take the medication with food to reduce the nausea. It is further explained that the nausea is likely to subside within a few days. A week later, when the pharmacist checks in with HB, she is tolerating the medication well, but is almost out having received only enough for two weeks. The pharmacist contacts the prescriber to initiate the dose escalation process to make sure HB reaches the minimum maintenance dose of 6mg daily. 19
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 4 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 20
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Continuous Monitoring for Drug and Disease State Interactions Few recommendations to avoid use with other medications due to interactions Rivastigmine o Not recommended to be used with beta antagonists due to risk of bradycardia Congestive heart failure (CHF), hypertension Risk is also inherent with use of other acetylcholinesterase inhibitors. o Concurrent use with metoclopramide is not recommended due to risk of additive extrapyramidal side effects. Gastrointestinal (GI) motility disorders, nausea Memantine o Use with caution in persons receiving other NMDA antagonists (amantadine, ketamine, dextromethorphan) due to the potential for adverse events with Parkinson’s disease, over-the-counter (OTC) cough and cold remedies 21
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Anticholinergic Load Pharmacists should monitor for the use of medications that can be antagonistic to the therapeutic effects of the cholinesterase inhibitors. o Anticholinergic medications may mitigate benefits. o Several easy-to-use scales are available to quantify estimated anticholinergic burden (e.g. Anticholinergic Cognitive Burden Scale, Anticholinergic Risk Scale). May also be used to gauge risk of dementia development as associated with anticholinergic exposure (J Am Ger Soc below). (Carnahan et al., 2006; Chew et al., 2008; Han et al., 2008; Boustani et al., 2008; Rudolph et al., 2008) 22
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Identification and Management of Comorbidities Psychiatric comorbidities eventually present in nearly all persons with dementia. Depression o Can use simple screening tools (e.g. Patient Health Questionnaire (PHQ)-2 or -9, Geriatric Depression Scale). Can also be used to monitor for medication effectiveness. Consider side effects that may be helpful for disease symptoms. Psychosis o Try non-medication interventions first due to increased morbidity and mortality in persons living with dementia exposed to antipsychotic therapy. o Ensure person is sleeping adequately as sleep deprivation may precipitate symptoms . o Continuously monitor for opportunities for medication discontinuation. Anxiety o Use antidepressants or short-acting antianxiety agents as needed. Agitation/aggressive behavior o As with psychosis, try non-drug therapy first. o May require acute, short-term use of behavior modifying medications (e.g. antipsychotics) if person is at risk of harm to self or others (Reus et al., 2016). 23
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Identification and Management of Comorbidities (continued) Common non-psychiatric comorbid conditions: Bladder/bowel dysfunction o Encourage regular toileting; time diuretic medications appropriately. o Suggest appropriate over-the-counter (OTC) products. Falls o Look for medications that do not increase the risk for falls. o Engage in discussions about and/or supply assistive devices. o Facilitate screening for bone loss and initiation of medications if appropriate. Infections o Advise appropriate use of vaccinations and administer if possible. o Monitor use of OTC medications. Sleep disturbances o Educate about behavioral strategies before suggesting OTC sleep aids. o Monitor for symptoms of excessive sedation, evaluate medications that affect sleep. 24
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 5 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 25
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Monitor for and Address Non-adherence Explore reasons for non-adherence. o Financial Direct to assistance programs. Suggest less expensive alternatives to drug therapy. Work with prescriber to eliminate unnecessary medications. o Difficulty remembering to take medication Explore electronic devices. Set up pill boxes for persons who have difficulty managing or remembering if they took their medication. Suggest reminder strategies (e.g. strategic placement of medication bottles). Encourage care partners to manage and supervise medication administration, especially for adults with Down syndrome or other intellectual disability. Package medication in bubble packs 26
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Monitor for and Address Non-adherence (continued) Need for alternate dosage form o Difficulty swallowing May suggest evaluation by a speech therapist be sought. o Frequency of use o Make sure instruction is given with regard to when manipulation of dosage forms is inadvisable. Adverse effects o Inquire about intolerable adverse effects. Educate about transient nature of side effect if applicable. Provide strategies to overcome if possible. Work with prescriber to find therapeutic alternative, or to decrease dose. Suggest additional medications to alleviate side effects. (Swallowing Disorders (Dysphagia) in Adults, 2016; Sadowsky et al., 2010) 27
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 6 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 28
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 The Pharmacist’s Role in Caring for Persons with Advancing Disease Pharmacists should continue to monitor for advancement of symptoms. o Inquire with care partners. o Suggest when it might be time to consider speaking to a prescriber about the advantages of continuing vs. discontinuing medication. o Consider speaking to prescribers about the possible discontinuation of maintenance medications that might be unnecessary in someone with advanced dementia. o Provide basic information about services such as hospice, or refer to those who can. (McGuffey, 1997; Mölsä, 1986; DeSimone & Viereck, 2011; Brookmeyer et al., 2007; Allgaier & Allgaier, 2013) 29
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Case Study Part 3 Several years pass, and HB is currently receiving rivastigmine 6mg by mouth twice daily, along with extended release memantine at a dose of 28mg by mouth daily. HB’s son now routinely picks up her prescriptions, as HB’s Alzheimer’s disease has progressed significantly, and she no longer recognizes her family nor is she able to leave the house safely. Upon talking to her son in more detail, the pharmacist becomes aware that HB will be entering hospice care. The pharmacist asks the son if he would like her to intervene with the prescriber to discuss some possible modifications to HB’s medication profile, including discontinuation of the medications that have been prescribed for Alzheimer’s disease, as well as her osteoporosis and cholesterol medications. The son agrees, and the pharmacist is successful in getting orders to discontinue the medications that are unlikely to enhance HB’s health to a substantial degree at this point in her disease. 30
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Outline 7 Identifying persons at risk for dementia Initiation of medication for the treatment of dementia Ongoing dementia management o Managing comorbid conditions o Identifying and addressing reasons for non-adherence o Approach to the person living with dementia with advancing disease Caring for the care partner 31
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Caring for the Care Partner Usually, anywhere from 1 to 4 family members act as care partners for a person with Alzheimer’s disease. o One person in 10 has a family member with Alzheimer’s disease. Care partner burden can result in harm for both that individual and the person living with dementia. o Watch for signs of substandard care, abuse or neglect. Care partners for adults with Down syndrome and other intellectual disabilities may be aging parents, siblings, or agency care personnel. Pharmacists should also monitor and question care partners for signs of depression and other mental/physical health issues, and facilitate intervention if necessary. (Terrie, 2016; Svendsboe et al., 2016) 32
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Evaluation 1. Which of the following is not applicable to the role of the pharmacist in identifying persons who should be evaluated for a diagnosis of dementia? a.Administer screening tests such as the Montreal Cognitive Assessment (MoCA). b.Diagnose the person and refer to a prescriber. c. Monitor for changes in patterns such as early requests for medication refills. d.Refer persons with memory loss to a dementia specialist. 2.Which is an appropriate approach to choosing medications for the treatment of a person living with dementia? a. Initiate therapy with galantamine as it has been proven to be the most effective medication. b. Consider memantine for monotherapy in persons living with mild dementia. c. Suggest a tricyclic antidepressant for person living with dementia who need treatment for depression. d. Consider rivastigmine for persons who have difficulty swallowing. 33
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Evaluation (Continued) 3. Select the true statement about medication monitoring for the person living with dementia. a.Persons living with dementia should be instructed to stop their dementia medication if they experience side effects, and discuss the problem at their next regularly schedule appointment. b.Medications for the treatment of Alzheimer’s disease should be titrated to the maximum tolerated approved dose. c.All OTC medications should be considered safe for use in the person living with dementia as there are no known drug or disease interactions that have been identified. d.If the person living with dementia is not showing signs of symptom reversal, a different medication should be chosen. 4. The person living with advanced or end-stage dementia e.Should have all non-dementia related medications discontinued. f.Should be placed on antipsychotic therapy for behavioral symptoms. g.Should be placed on dual cholinesterase inhibitor therapy to offset their high cholinergic deficit. h.Should be screened for unnecessary maintenance medications unrelated to the diagnosis of dementia. 34
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Acknowledgements This module was prepared for the U.S. Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA), by The Bizzell Group, LLC., under contract number HHSH25034002T/HHSH250201400075I. The dementia and education experts who served on the Dementia Expert Workgroup to guide the development of the modules included: Alice Bonner, PhD, RN, FAAN, Secretary Elder Affairs, Massachusetts Executive Office of Elder Affairs, Boston MA; Laurel Coleman, MD, FACP, Kauai Medical Clinic -Hawaii Pacific Health, Lihue, HI; Cyndy B. Cordell, MBA, Director, Healthcare Professional Services, Alzheimer's Association, Chicago, IL; Dolores Gallagher Thompson, PhD, ABPP, Professor of Research, Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine, Stanford, CA; James Galvin, MD, MPH, Professor of Clinical Biomedical Science and Associate Dean for Clinical Research, Florida Atlantic University, Boca Raton, FL; Mary Guerriero Austrom, PhD, Wesley P Martin Professor of Alzheimer's Disease Education, Department of Psychiatry, Associate Dean for Diversity Affairs, Indiana University-Purdue University Indianapolis, Indianapolis, IN; Robert Kane, MD, Professor and Minnesota Chair in Long-term Care & Aging, Health Policy & Management, School of Public Health, University of Minnesota; Jason Karlawish, MD, Professor of Medicine, Perelman School of Medicine, University of Pennsylvania; Helen M. Matheny, MS, APR, Director of the Alzheimer's Disease Outreach Program, Blanchette Rockefeller Neuroscience Institute, Morgantown, WV; Darby Morhardt, PhD, LCSW, Associate Professor, Cognitive Neurology and Alzheimer's Disease Center and Department of Preventive Medicine, Northwestern University Feinberg School of Medicine, Northwestern University, Chicago, IL; Cecilia Rokusek, EdD, MSc, RDN, Assistant Dean of Research and Innovation, Professor of Family Medicine, Public Health, Nutrition, and Disaster and Emergency Preparedness, College of Osteopathic Medicine, Nova Southeastern University, Fort Lauderdale, FL. Additional expertise in the development of the modules was provided by Meg Kabat, LCSW-C, CCM; Eleanor S. McConnell, PhD, MSN, RN, GCNS, BC; Linda O. Nichols, PhD, MA, BA; Todd Semla, MS, PharmD, BCPS, FCCP, AGSF; Kenneth Shay, DDS, MS, from the U.S. Department of Veterans Affairs and Seth Keller, MD and Matthew P. Janicki, PhD, National Task Group on Intellectual Disabilities and Dementia Practices. 35
MODULE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Brought to you by the U.S. Department of Health and Human Services, Health Resources and Services Administration 36