Multiple Sclerosis Disease of the Central Nervous System Presented by:




31 Slides970.00 KB
Multiple Sclerosis Disease of the Central Nervous System Presented by: Dana Hogan RN, BSN Teresa Pearson RN, BSN Kristin Poage RN, BSN Laura Webb RN, BSN
Multiple Sclerosis: Definition Multiple Sclerosis (MS) is a chronic autoimmune demyelination disease of the central nervous system (CNS) characterized by clinical attacks correlated with lesions separated in time and space. (Ferri’s, 2013).
Epidemiology » PEAK INCIDENCE: 20 to 40 years of age. » PREVALANCE: MS is more common in people raised in northern latitudes and in certain genetic clusters. » PREDOMINANT SEX & AGE: Female/male ratio is 2 to 3:1 » GENETICS: Frequency of MS in Dizygotic Twins & Monozygotic twins. (Department of Neurology and Research) Multiple Sclerosis
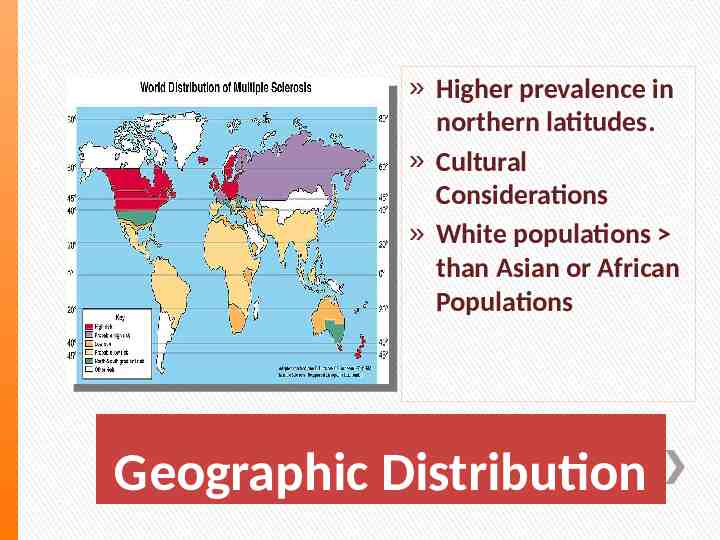
» Higher prevalence in northern latitudes. » Cultural Considerations » White populations than Asian or African Populations Geographic Distribution
» The precise etiology of MS is uncertain. There is evidence that autoimmunity (autoreacitve T cells and B cells) plays an important role. It is believed that an interaction between multiple genes influencing the immune system and environmental factors such as certain viruses e.g. Epstein-Barr virus and human herpes virus 6, low Vitamin D level, smoking, and sun exposure are important factors. (Ferri’s, 2013). Etiology MS
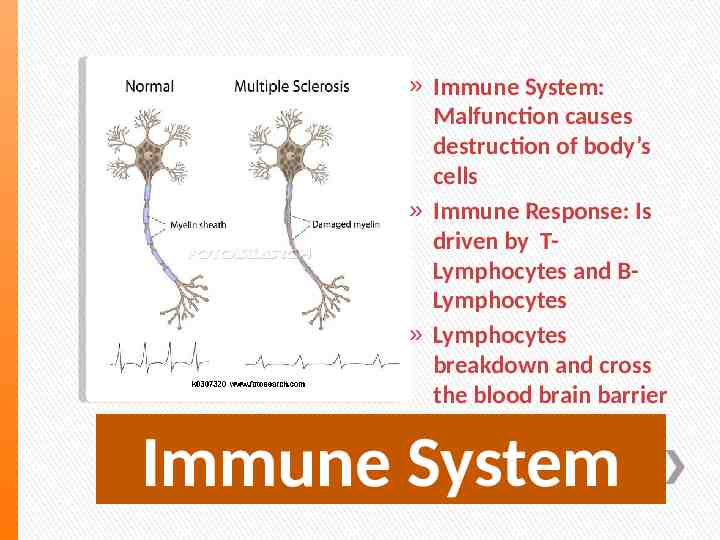
» Immune System: Malfunction causes destruction of body’s cells » Immune Response: Is driven by TLymphocytes and BLymphocytes » Lymphocytes breakdown and cross the blood brain barrier Immune System
CNS Review
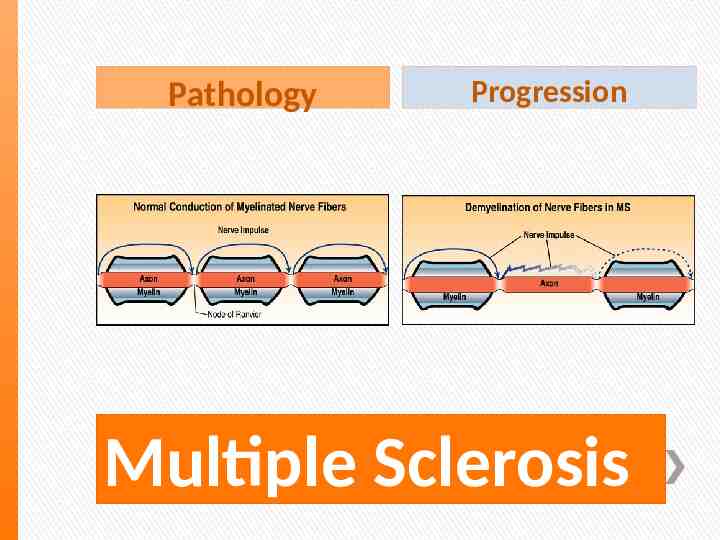
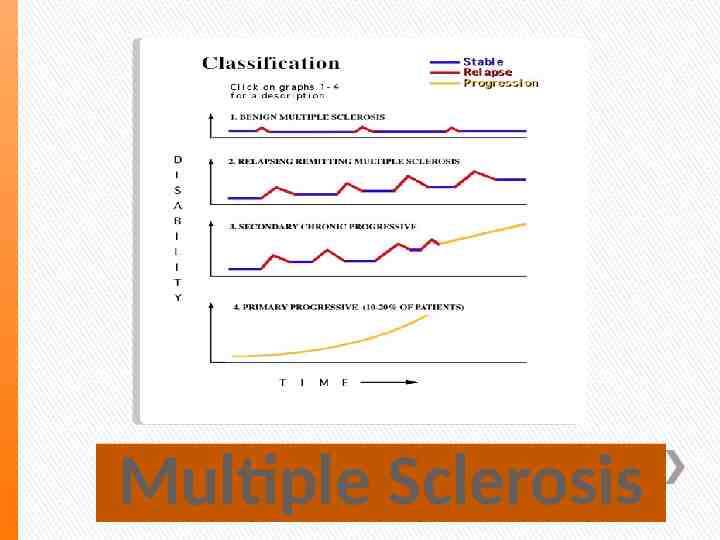
Pathology Progression Multiple Sclerosis
Pathology » MS is a nerve disorder caused by destruction of the insulating layer surrounding neurons in the brain and spinal cord. Myelin helps electrical signals pass quickly and smoothly between the brain and the rest of the body. When the Myelin is destroyed, nerve messages are sent more slowly and less efficiently. » Oligodendrocytes-Glial Cells » Nerve Cells Disruption Destruction of Myelin
» Subtypes include: Basic Information Relapsing-Remitting MS (RRMS), Most Common Secondary Progressive MS (SPMS) Primary Progressive MS (PPMS) Progressive Relapsing MS (PRMS) Neuromyelitis Optica (NMO: Devic’s Disease) Marburg’s Disease (Malignant MS) Balo’s Concentric Sclerosis Schilder’s Diffuse Sclerosis Relapsing Optic Neuritis (Ferri’s, 2013)
Multiple Sclerosis
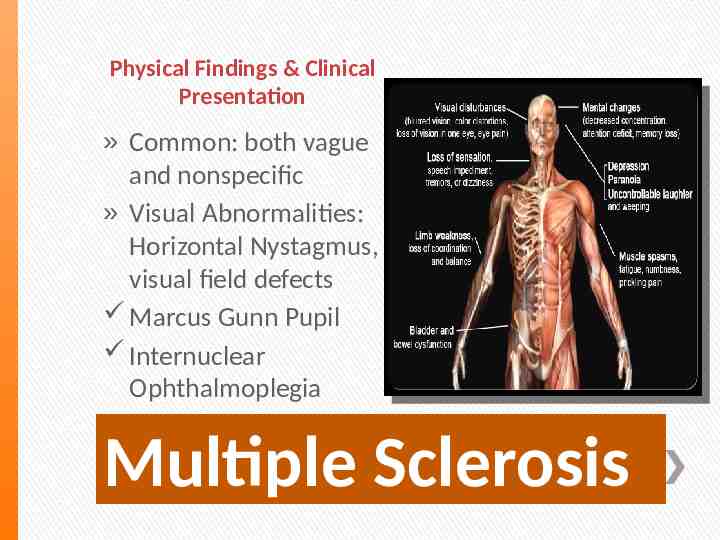
Physical Findings & Clinical Presentation » Common: both vague and nonspecific » Visual Abnormalities: Horizontal Nystagmus, visual field defects Marcus Gunn Pupil Internuclear Ophthalmoplegia Multiple Sclerosis
Physical Findings and Clinical Presentation » Corticospinal Tract Involvement » Sensory Loss » Ataxia » Bladder Dysfunction » Lhermitte’s Sign » Uhtoff’s Phenomenon Continued
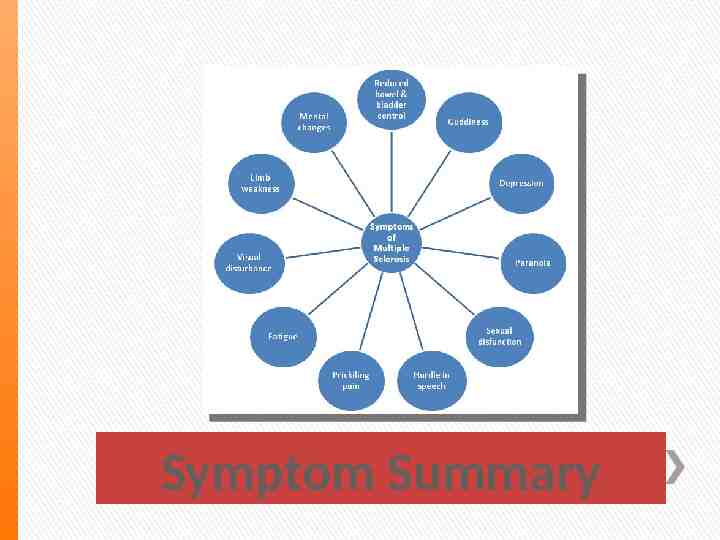
Symptoms » Early: Numbness in 1or more limbs, partial paralysis, double or blurred vision in 1 eye » Later: Loss of coordination, loss of ability to walk of bladder or bowel control » Mental Symptoms: Depression, forgetfulness, loss of concentration Multiple Sclerosis
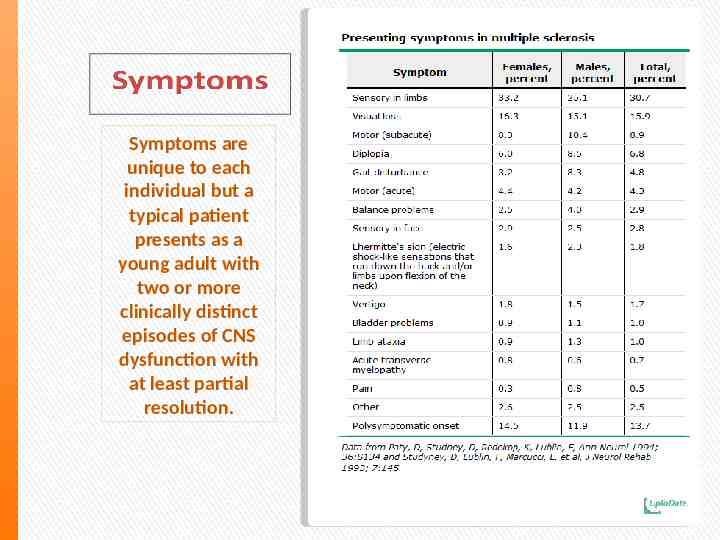
Symptoms are unique to each individual but a typical patient presents as a young adult with two or more clinically distinct episodes of CNS dysfunction with at least partial resolution.
Symptom Summary
Differential Diagnosis Differential Diagnosis » Autoimmune: Acute Disseminated Encephalomyelitis (ADEM), Postvaccination Encephalomyelitis » Degenerative: Subacute Combined Degeneration of the cord (B-12 deficiency), Amyotrophic lateral sclerosis » Infections: Lyme’s Disease, Neurosyphillis, HIV, Tropical Spastic Paraparesis, Progressive Multifocal Leukoencephalopahty, Whipple’s Disease » Inflammatory: Systemic Lupus, Erythematosus, Vasculitis, Sarcoidosis, » Sjogren’s Disease, Behcet’s Disease, Celiac Disease » Mitochondrial: Leber’s Hereditary Optic Neuropathy, Mitochondrial Encephalopathy, Lactic Acidosis, and Stroke-like Episodes DX:
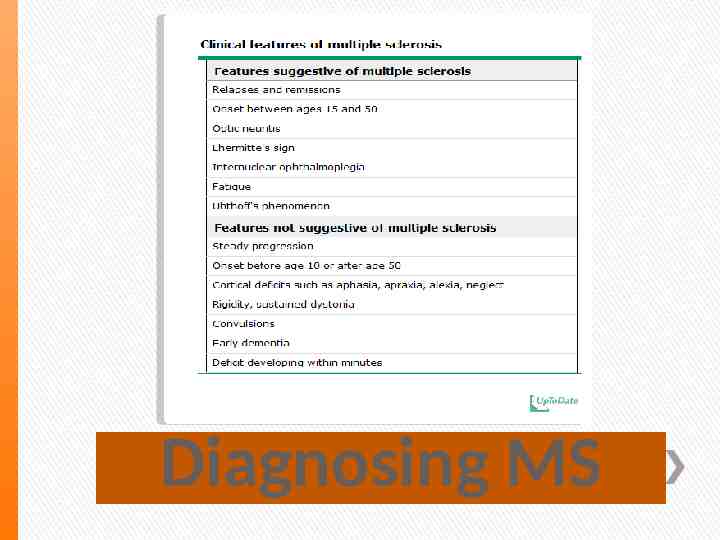
Diagnosing MS
» MS is a clinical diagnosis, based on symptoms of an “attack”. » An MS attack (also called a relapse or exacerbation) is defined by the McDonald criteria as patient-reported or objectively observed event typical of an acute inflammatory demyelinating event in the CNS, and can be either current or historical, with duration of at least 24 hours, in the absence of fever or infection. » MRI of brain and spine is then done and the McDonald’s criteria, based on symptoms and lesions found and their location a supportive diagnosis of Multiple Sclerosis can be made. Diagnosing MS
» » » » » OLD CARTS Family history of MS? Smoker? Past medical history of cerebral spinal fluid problems? EXAM: Neurologic HEENT Respiratory Cardiac Musculoskeletal Genitourinary Abdominal Psychiatric Constitutional Diagnosing MS
» RRMS: At least two relapses-two clinical lesions distinctly separated in space and time or one clinical lesion plus paraclinical testing » PPMS: Insidious progression of disability with a positive CSF and either dissemination in both space and time or ongoing progression for at least 1 year. Diagnosis: McDonald Criteria
» Lumbar Puncture: All first-line relapses and all cases in which the DX of MS is not DEFINITE. » Serum: Complete Blood Count (CBC), Sedimentation Rate (Sed-rate), CHEM 7, Liver function tests (LFT’s), Antinuclear Antibody, and Vit.-B 12. » Consider: Anti-SS-A antibody, Anti-SS-B antibody, Neuromyelitis Optica IgG antibody, Lyme Titer, Angiotension-Coverting Enzyme, TSH, Free T-4, AntiThyroglobulin antibody, Very Long-Chain Fatty Acid, Arylsulfatase A, and Possibly Heavy Metal Screening (Urine) » Head Imaging (CT or MRI) is strongly recommended. MS Workup
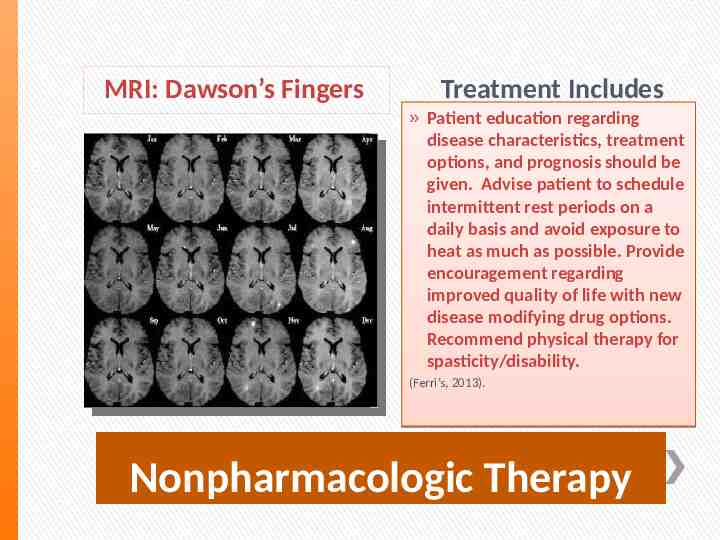
MRI: Dawson’s Fingers Treatment Includes » Patient education regarding disease characteristics, treatment options, and prognosis should be given. Advise patient to schedule intermittent rest periods on a daily basis and avoid exposure to heat as much as possible. Provide encouragement regarding improved quality of life with new disease modifying drug options. Recommend physical therapy for spasticity/disability. (Ferri’s, 2013). Nonpharmacologic Therapy
» Relapses: High-Dose IV Methylprednisone (3 to 5 days), alternative is 15 mg/kg/day), followed by a 7-10 day prednisone taper. » If marked acute disability and acute corticosteroid therapy has failed, plasma exchange (5-7 exchanges on alternate days) have shown benefit. (Ferri’s, 2013) Acute General RX
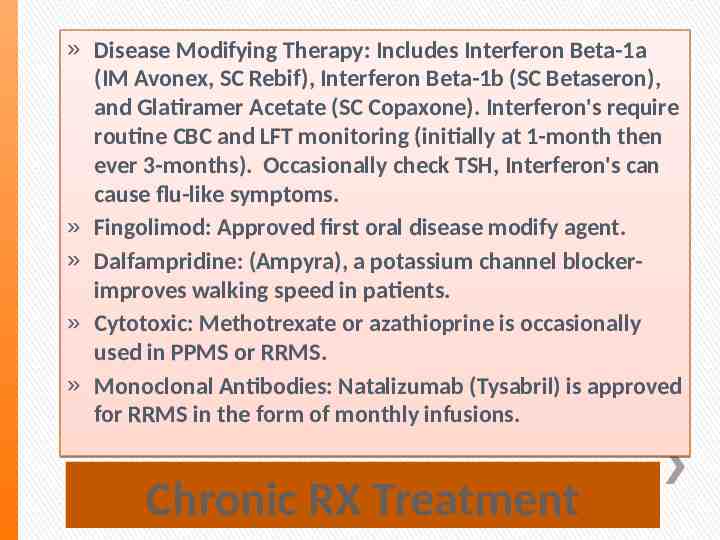
» Disease Modifying Therapy: Includes Interferon Beta-1a (IM Avonex, SC Rebif), Interferon Beta-1b (SC Betaseron), and Glatiramer Acetate (SC Copaxone). Interferon's require routine CBC and LFT monitoring (initially at 1-month then ever 3-months). Occasionally check TSH, Interferon's can cause flu-like symptoms. » Fingolimod: Approved first oral disease modify agent. » Dalfampridine: (Ampyra), a potassium channel blockerimproves walking speed in patients. » Cytotoxic: Methotrexate or azathioprine is occasionally used in PPMS or RRMS. » Monoclonal Antibodies: Natalizumab (Tysabril) is approved for RRMS in the form of monthly infusions. Chronic RX Treatment
Chronic Continued » Pain: Carbamazepine, Gabapentin, or Amitriptyline » Fatigue: Consider Amantadine 100mg BID, Modafinil (most effective for somnolence), or Fluoxetine Clay Walker
Referral » Referral to neurology on DX is highly recommended. » Consider referrals for PT, and OT to prevent/minimize disability. » Consider referral to urology if post-void residual by bladder scan is more than 100 ml. » Referral to MS specialist should be strongly considered in case of poor response to therapy, possibility of cytotoxic treatment, and /or concern regarding accuracy of diagnosis (Ferri’s, 2013) Multiple Sclerosis
Multiple Sclerosis Question # 1 » A 34 y/o female has been recently DX with Multiple Sclerosis (MS). When providing primary care for this patient, you consider that MS: A. Has a predictable course of progressive decline in intellectual and motor function. B. Manifests with a classic pattern of Myalgia, blurred vision, and Ataxia. C. Is often seen with a variable pattern of exacerbation and remissions. D. Is accompanied by classic central nervous system lesions detectable on skull films. ANSWER: C Review .
» Treatment options in MS to attenuate disease progression include: A. Interferon beta1b B. Methylprednisolo ne C. Ribavirin D. Phenytoin ANSWER: A Questions # 2
Question #3: Current pharmacological therapy for chronic relapsing-remitting multiple sclerosis involves .
A: High-Dose Steroids B: Baclofen or Diazepam C: Interferon B (Betaseron) D: Benzodiazepines