Fundamentals of Nursing(1st Stage) Bowel Elimination Lecture


























27 Slides326.37 KB
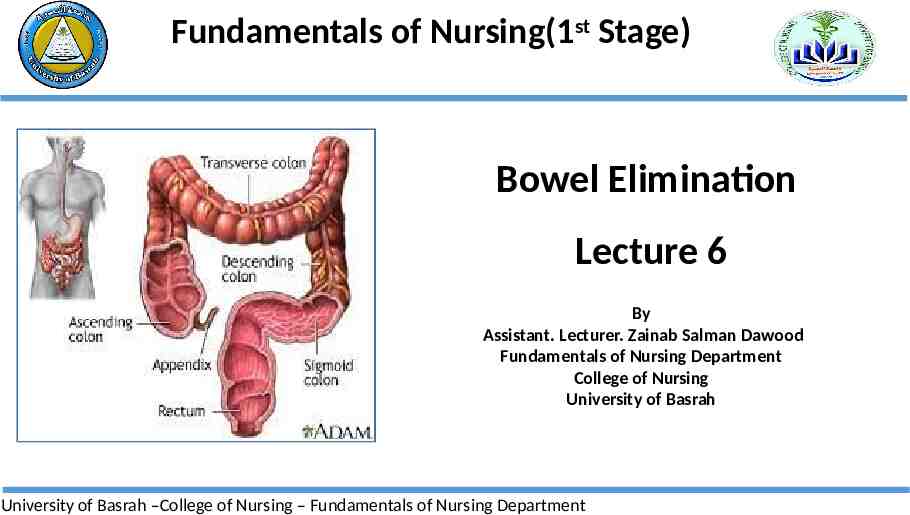
Fundamentals of Nursing(1st Stage) Bowel Elimination Lecture 6 By Assistant. Lecturer. Zainab Salman Dawood Fundamentals of Nursing Department College of Nursing University of Basrah University of Basrah –College of Nursing – Fundamentals of Nursing Department
Introduction Expectations about bowel elimination, usual patterns of defecation, and the ease with which a person speaks about bowel problems differ widely among people. Although most people have experienced minor acute bouts of diarrhea or constipation, some people experience severe or chronic alterations in bowel elimination that affect their fluid and electrolyte balance, hydration, nutritional status, skin integrity, comfort, and selfconcept. University of Basrah –College of Nursing– Fundamentals of Nursing Department
Gastrointestinal Tract The gastrointestinal tract, also known as the alimentary tract or canal extends from the mouth to the anus. The major organ involved with bowel elimination is the large intestine. University of Basrah –College of Nursing– Fundamentals of Nursing Department
large intestine The primary organ of bowel elimination, is the lower, or distal, part of the gastrointestinal tract. The large intestine, also known as the colon, extends from the ileocecal valve to the anus. The colon in adults is about 1.5 m long, but variations in length are normal. Width also varies; at its narrowest point, the colon is about 2.5 cm wide; at its widest point, it is about 7.5 cm. The diameter of the colon decreases from the cecum to the anus University of Basrah –College of Nursing– Fundamentals of Nursing Department
large intestine The connection between the ileum of the small intestine and the large intestine is the ileocecal, or ileocolic valve. This valve normally prevents contents from entering the large intestine prematurely and prevents waste products from returning to the small intestine. University of Basrah –College of Nursing– Fundamentals of Nursing Department
From the cecum, the first part of the large intestine, the digestive contents enter the colon, which consists of several segments. The ascending colon extends from the cecum upward toward the liver, where it turns to cross the abdomen. This turn is called the hepatic flexure. Upon turning, this portion of the colon becomes the transverse colon, crossing the abdomen from right to left. The colon then turns at the splenic flexure to become the descending colon. The descending colon passes down the left side of the body to the sigmoid, or pelvic, colon. University of Basrah –College of Nursing– Fundamentals of Nursing Department
University of Basrah –College of Nursing– Fundamentals of Nursing Department
The sigmoid colon contains feces, solid waste products that have reached the distal end of the colon and are ready for excretion. Once excreted, feces are called stool. The sigmoid colon empties into the rectum, the last part of the large intestine. The rectum is about 12 cm long, 2.5 cm of which is the anal canal. The rectum is empty except immediately before and during defecation (the process of bowel elimination; a bowel movement). Feces are excreted from the rectum through the anal canal, and out an opening called the anus. University of Basrah –College of Nursing– Fundamentals of Nursing Department
University of Basrah –College of Nursing– Fundamentals of Nursing Department
Functions of the large intestine 1. 2. 3. 4. Absorption of water Formation of feces Expulsion of feces from the body. Bacteria that reside in the large intestine act on food residue while it makes its way through the large intestine. 5. Bacterial action produces vitamin K and some of the Bcomplex vitamins. University of Basrah –College of Nursing– Fundamentals of Nursing Department
Defecation Defecation refers to the emptying of the large intestine. Two centers govern the reflex to defecate, one in the medulla and a subsidiary one in the spinal cord. When parasympathetic stimulation occurs, the internal anal sphincter relaxes and the colon contracts, allowing the fecal mass to enter the rectum. The rectum becomes distended by the fecal mass, the primary stimulus for the defecation reflex. Rectal distention leads to an increase in intra-rectal pressure, causing the muscles to stretch and thereby stimulating the defecation reflex and subsequently the urge to eliminate. University of Basrah –College of Nursing– Fundamentals of Nursing Department
FACTORS AFFECTING BOWEL ELIMINATION 1- Developmental Considerations Age affects what a person eats and the body’s ability to digest nutrients and eliminate wastes. The stools of an infant are markedly different from those of an older person. Because patients are often reluctant to discuss their bowel habits and stool characteristics, nurses need to be familiar with bowel concerns pertinent to each developmental group. University of Basrah –College of Nursing– Fundamentals of Nursing Department
2- Daily Patterns Most people have individual patterns of bowel elimination involving frequency, timing considerations, position, and place. Changes in any of these patterns may upset a person’s routine and lead to constipation. University of Basrah –College of Nursing– Fundamentals of Nursing Department
3- Food and Fluid Both the type and the amount of foods eaten and the amount of fluids ingested affect elimination. A high-fiber diet and a daily fluid intake of 2,000 to 3,000 mL facilitate bowel elimination. High-fiber foods, such as whole grains and bran, dried peas and beans, and fresh fruits and vegetables, increase the bulk in fecal material. Bulkier feces increase pressure on the intestinal wall, which serves as a stimulus for peristalsis. University of Basrah –College of Nursing– Fundamentals of Nursing Department
4- Activity and Muscle Tone Regular exercise improves gastrointestinal motility and muscle tone, whereas inactivity decreases both. Adequatetone in the abdominal muscles, the diaphragm, and the perineal muscles is essential for ease of defecation. Patients on prolonged bed rest or those with decreased mobility are prime candidates for constipation. University of Basrah –College of Nursing– Fundamentals of Nursing Department
5- Lifestyle Many individual, family, and sociocultural variables influence a person’s usual elimination habits. The long term effects of bowel training may result in a person’s : (1) Acceptance of bowel elimination as a normal life process (2) Preoccupation with bowel elimination. (3) Feeling that bowel elimination is a “dirty” process. University of Basrah –College of Nursing– Fundamentals of Nursing Department
6- Psychological Variables Psychological stress affects the body in many ways. In some people, anxiety seems to have a direct effect on gastrointestinal motility, and diarrhea accompanies periods of high anxiety. University of Basrah –College of Nursing– Fundamentals of Nursing Department
7- Pathologic Conditions Numerous pathologic processes may change a person’s usual bowel elimination habits. Changes in stool characteristics or frequency may be one of the first clinical manifestations of a disease; their evaluation may lead to the diagnosis of the disease. For example, when a patient reports stool has become narrower or ribbon-like, a tumor may be obstructing normal stool passage through the colon. University of Basrah –College of Nursing– Fundamentals of Nursing Department
8- Medications Medications are available that can promote peristalsis (cathartics and laxatives) or inhibit peristalsis (antidiarrheal medications). University of Basrah –College of Nursing– Fundamentals of Nursing Department
9- Diagnostic Studies Diagnostic studies may affect a patient’s usual bowel elimination pattern. For example, patients may need to fast for diagnostic studies. The ingestion of barium during diagnostic procedures, such as a barium enema, may result in constipation or impaction if it is not completely eliminated after the procedure. University of Basrah –College of Nursing– Fundamentals of Nursing Department
10-Surgery and Anesthesia Abdominal incisions and direct manipulation of the bowel during abdominal surgery inhibit peristalsis, causing a condition termed paralytic ileus (postoperative ileus). This temporary stoppage of peristalsis normally lasts 3 to 5 days. University of Basrah –College of Nursing– Fundamentals of Nursing Department
Constipation occurs when bowel movements become less frequent than normal. It is accompanied by a difficult or incomplete passage of stool.
Nursing Interventions Encourage the patient to take in fluid 2000 to 3000 mL/day, if not contraindicated medically. Assist patient to take at least 20 g of dietary fiber (e.g., raw fruits, fresh vegetable, whole grains) per day. Urge patient for some physical activity and exercise. Consider isometric abdominal and gluteal exercises. Encourage a regular period for elimination. Using the heel of the hand or a tennis ball, apply and release pressure firmly but gently around the abdomen in a clockwise direction. University of Basrah –College of Nursing– Fundamentals of Nursing Department
Diarrhea is an increase in the frequency of bowel movements, as well as the water content and volume of the waste University of Basrah –College of Nursing– Fundamentals of Nursing Department
Nursing Interventions Weigh patient daily and note decreased weight. Have patient keep a diary that includes the following: time of day defecation occurs; usual stimulus for defecation; consistency, amount, and frequency of stool. Avoid using medications that slow peristalsis. Give antidiarrheal drugs as ordered. University of Basrah –College of Nursing– Fundamentals of Nursing Department
Record number and consistency of stools per day. Evaluate dehydration by observing skin turgor over sternum and inspecting for longitudinal furrows of the tongue. Watch for excessive thirst, fever, dizziness, lightheadedness, palpitations, excessive cramping, bloody stools, hypotension, and symptoms of shock. Encourage fluids 1.5 to 2 L/24 hr plus 200 mL for each loose stool in adults unless contraindicated; consider nutritional support. Monitor and record intake and output; note oliguria and dark, concentrated urine.
Thanks