Creating a HIV Pre-exposure Prophylaxis (PrEP) Clinic at


64 Slides4.58 MB
Creating a HIV Pre-exposure Prophylaxis (PrEP) Clinic at a College Health Service ACHA Annual Meeting, Austin, Texas Friday, June 2, 2017 – 10:00 – 11:30 AM Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine President-elect, American College Health Association Sterling LaBoo Texas A&M University
GREETINGS FROM Emory University and Texas A&M University
Faculty Disclosure Neither presenter has a financial interest, arrangement or affiliation with any organization or business entity (including self-employment or sole proprietorship) that could be perceived as a conflict of interest or source of bias in the context of this presentation.
Learning Objectives Discuss the literature supporting the use of antiretroviral medication for pre-exposure HIV prophylaxis (PrEP). Discuss the controversies surrounding the use of PrEP as a public health strategy. Describe the indications for PrEP. Describe steps to take to create an HIV PrEP clinic in a college health setting. To meet Pharmacist Continuing Education Requirements, we will be doing Knowledge Assessments and Discussion Topics throughout this presentation!
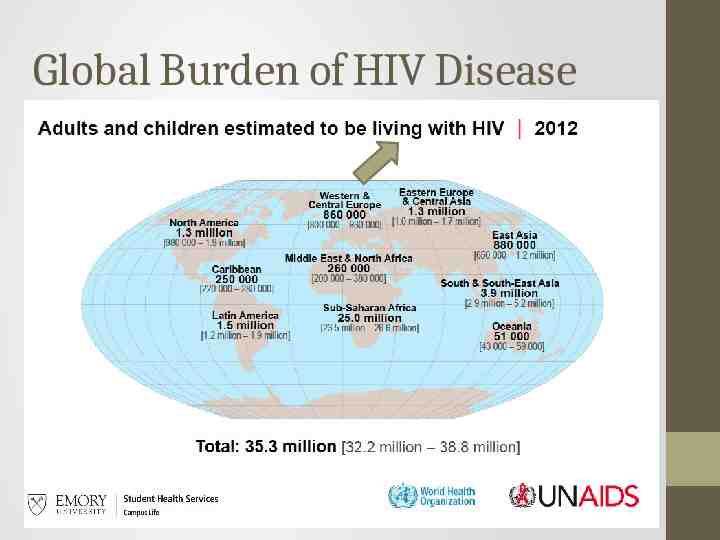
Global Burden of HIV Disease
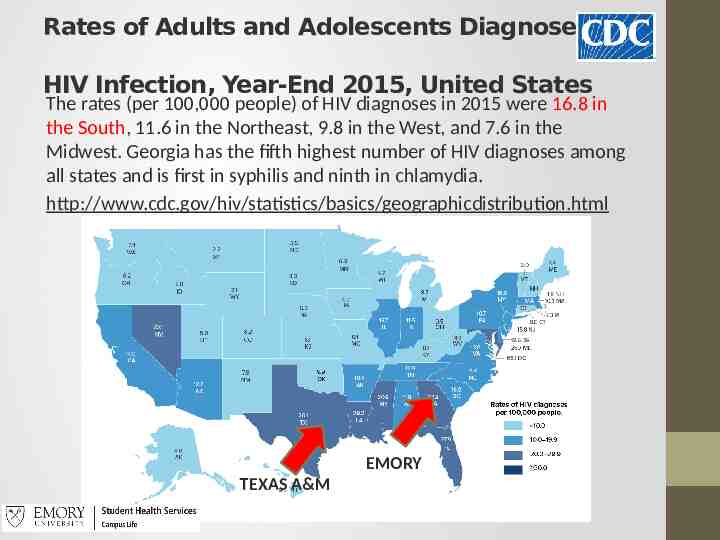
Rates of Adults and Adolescents Diagnoses of HIV Infection, Year-End 2015, United States The rates (per 100,000 people) of HIV diagnoses in 2015 were 16.8 in the South, 11.6 in the Northeast, 9.8 in the West, and 7.6 in the Midwest. Georgia has the fifth highest number of HIV diagnoses among all states and is first in syphilis and ninth in chlamydia. http://www.cdc.gov/hiv/statistics/basics/geographicdistribution.html Atlanta EMORY TEXAS A&M
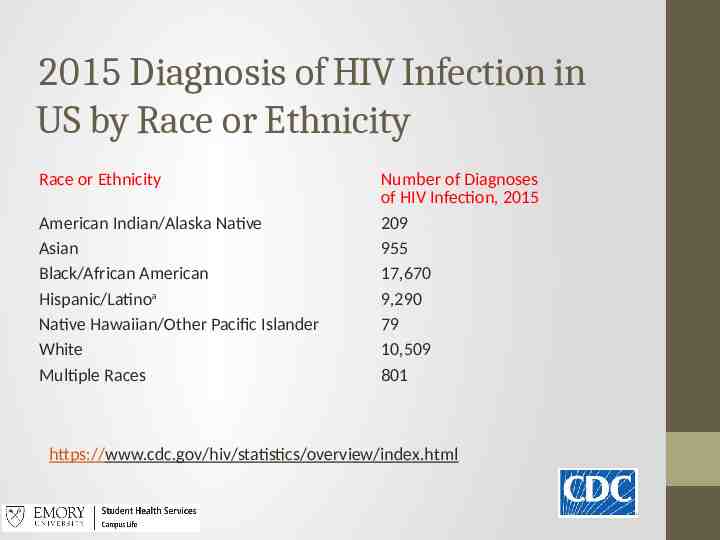
2015 Diagnosis of HIV Infection in US by Race or Ethnicity Race or Ethnicity American Indian/Alaska Native Asian Black/African American Hispanic/Latinoa Native Hawaiian/Other Pacific Islander White Multiple Races Number of Diagnoses of HIV Infection, 2015 209 955 17,670 9,290 79 10,509 801 https://www.cdc.gov/hiv/statistics/overview/index.html
Black MSM in Atlanta (2014) Prevalence of HIV among black men who have sex with men (MSM) in Atlanta 40% compared to 15% in white MSM Incidence of HIV infection/year of young black MSM ( 25 years) in Atlanta 12% Individual levels of risk behavior do not completely explain this disparity
Social Determinants of Health as Drivers in the HIV Epidemic Social Determinants of Health (SDHs) are conditions, environments, social practices and attitudes that can shape the ways in which people are born, grow, live work, play, worship and age. A map of race, poverty and healthcare access in Atlanta almost exactly matches a map of HIV prevalence. Economic inequality in Atlanta is a SDH. Historical realities must be considered when addressing the geographic overlap between high HIV and high poverty prevalence.
HIV at Emory A college is not an island. After many years of no positive HIV tests (and the discontinuation of anonymous testing), in 2012 Emory SHS began seeing HIV tests in MSM-identified students and young male students still in a questioning phase. Many of the new cases were in young African American MSM. Students began asking about PrEP (HIV Pre-exposure Prophylaxis)
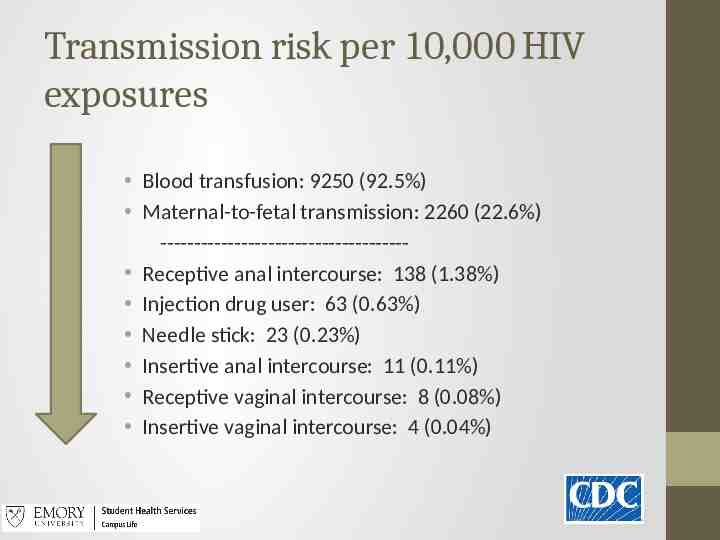
Transmission risk per 10,000 HIV exposures Blood transfusion: 9250 (92.5%) Maternal-to-fetal transmission: 2260 (22.6%) ------------------------------------ Receptive anal intercourse: 138 (1.38%) Injection drug user: 63 (0.63%) Needle stick: 23 (0.23%) Insertive anal intercourse: 11 (0.11%) Receptive vaginal intercourse: 8 (0.08%) Insertive vaginal intercourse: 4 (0.04%)
PrEP Daily oral medication [Tenofovir (TDF)/ Emtricitabine (FTC)] approved by FDA in 2010 for prevention of HIV infection in high risk individuals
Human PrEP Efficacy Studies 39 Randomized controlled trials 1987-2009 Enrolled 160,000 participants, mostly in Africa Standard measures of HIV prevention (education, condoms, STI screening/ treatment) are not highly effective at reducing HIV transmission However, PrEP prevention interventions (provided to both PrEP and control arms) was effective Adherence: If you take the medication, it is more likely to work
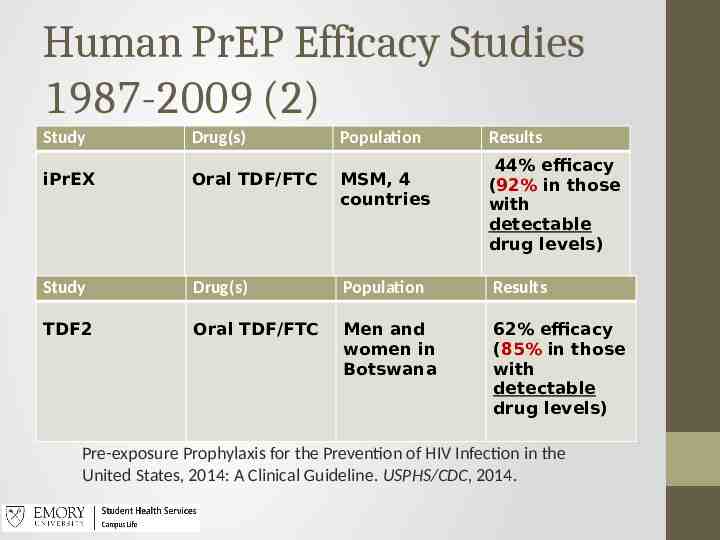
Human PrEP Efficacy Studies 1987-2009 (2) Study Drug(s) Population Results 44% efficacy (92% in those with detectable drug levels) iPrEX Oral TDF/FTC MSM, 4 countries Study Drug(s) Population Results TDF2 Oral TDF/FTC Men and women in Botswana 62% efficacy (85% in those with detectable drug levels) Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014.
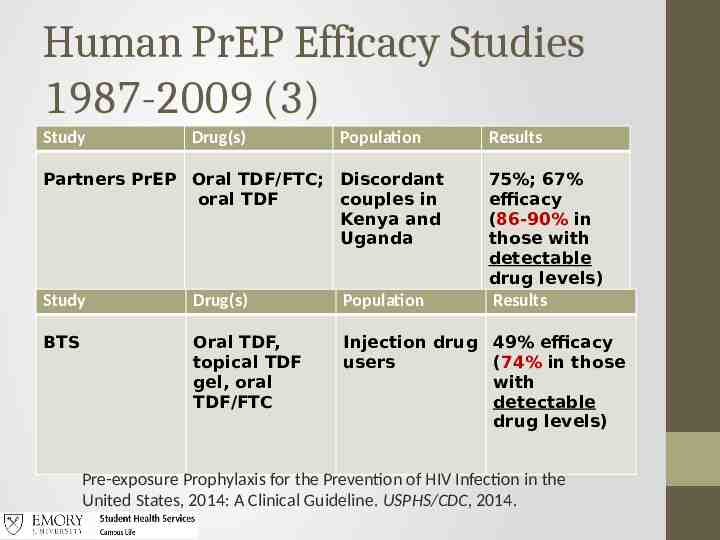
Human PrEP Efficacy Studies 1987-2009 (3) Study Drug(s) Population Results Partners PrEP Oral TDF/FTC; Discordant oral TDF couples in Kenya and Uganda 75%; 67% efficacy (86-90% in those with detectable drug levels) Study Drug(s) Population Results BTS Oral TDF, topical TDF gel, oral TDF/FTC Injection drug 49% efficacy users (74% in those with detectable drug levels) Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014.
The results are compelling. . . Data has shown an up to 92% reduction in HIV incidence in MSM adhering to a daily PrEP Rx regimen. While the CDC strongly recommends the prescribing of PrEP in primary care, and MSM college students are clearly interested, very few college health services are taking the steps to begin prescribing PrEP. If your students have not already asked you for a PrEP program at your SHS, they likely will soon. With a thoughtful and careful approach, appropriate infectious diseases consultant back-up, and adequate primary care and health promotion capabilities, HIV PrEP medication can be managed in many college health settings.
Knowledge Assessment #1 In human PrEP efficacy studies, what was the most important determinant of efficacy? 1. Adherence to the daily medication regimen. 2. Maintaining proper storage (temperature and humidity control) of the TDF/FTC medication. 3. Gender of the individual on TDF/FTC. 4. All of the above.
Knowledge Assessment #1 In human PrEP efficacy studies, what was the most important determinant of efficacy? 1. Adherence to the daily medication regimen. 2. Maintaining proper storage (temperature and humidity control) of the TDF/FTC medication. 3. Gender of the individual on TDF/FTC. 4. All of the above.
Knowledge Assessment #2 Rank the following HIV transmission risk factors in order, from highest risk of transmission to lowest risk of transmission: 1. 2. 3. 4. 5. Needle stick Receptive anal intercourse Blood transfusion Injection drug user Receptive vaginal intercourse
Knowledge Assessment #2 Rank the following HIV transmission risk factors in order, from highest risk of transmission to lowest risk of transmission: Per 10,000 HIV Exposures: 3, 2, 4, 1, 5 Blood transfusion: 9250 (92.5%) Receptive anal intercourse: 138 (1.38%) Injection drug user: 63 (0.63%) Needle stick: 23 (0.23%) Receptive vaginal intercourse: 8 (0.08%)
Steps to Create a PrEP Clinic at a College Health Service
Goal of a College Health PrEP Clinic Goal: Reduce the acquisition of HIV infection in our college/university students Prescribe medication regimen that are proven safe and effective for uninfected persons who meet recommended criteria Educate patients about the medications and regimen to maximize safe use Provide support for medication adherence Monitor patients to detect HIV infection, medication toxicities, and assess levels of risk behavior
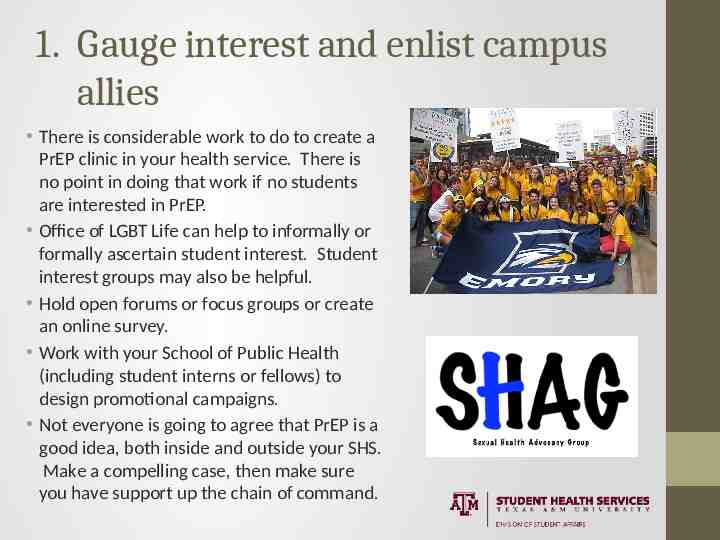
1. Gauge interest and enlist campus allies There is considerable work to do to create a PrEP clinic in your health service. There is no point in doing that work if no students are interested in PrEP. Office of LGBT Life can help to informally or formally ascertain student interest. Student interest groups may also be helpful. Hold open forums or focus groups or create an online survey. Work with your School of Public Health (including student interns or fellows) to design promotional campaigns. Not everyone is going to agree that PrEP is a good idea, both inside and outside your SHS. Make a compelling case, then make sure you have support up the chain of command.
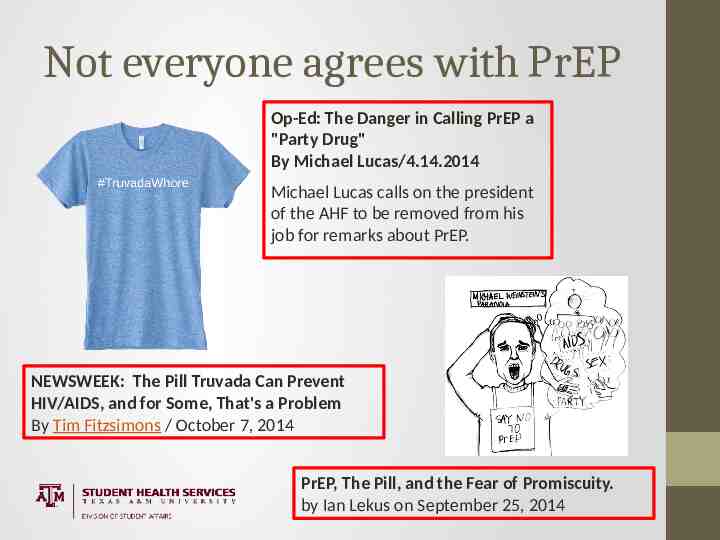
Not everyone agrees with PrEP Op-Ed: The Danger in Calling PrEP a "Party Drug" By Michael Lucas/4.14.2014 Michael Lucas calls on the president of the AHF to be removed from his job for remarks about PrEP. NEWSWEEK: The Pill Truvada Can Prevent HIV/AIDS, and for Some, That's a Problem By Tim Fitzsimons / October 7, 2014 PrEP, The Pill, and the Fear of Promiscuity. by Ian Lekus on September 25, 2014
Sound familiar? 1916 Margaret Sanger opens first birth control clinic in the United States. The next year she was deemed guilty of maintaining a public nuisance and sentenced to jail for 30 days. Once released, she re-opened her clinic and continued to persevere through more arrests and prosecutions. 1938 In a case involving Margaret Sanger, a judge lifted the federal ban on birth control, ending the Comstock era. Diaphragms, also known as womb veils, became a popular method of birth control. 1950 While in her 80s, Sanger underwrote the research necessary to create the first human birth control pill. She raised 150,000 for the project
Sound familiar (2)? 1960 The first oral contraceptive, Enovid, was approved by the US Food and Drug Administration (FDA) as contraception. 1965 The Supreme Court (in Griswold v. Connecticut) gave married couples the right to use birth control, ruling that it was protected in the Constitution as a right to privacy. However, millions of unmarried women in 26 states were still denied birth control. 1972 The Supreme Court (in Baird v. Eisenstadt) legalized birth control for all citizens of this country, irrespective of marital status. http://www.ourbodiesourselves.org/health-info/a-brief-history-of-birth-control/
2. Create a partnership between Primary Care and Health Promotion The PrEP efficacy studies involved an aggressive health education component to reduce high-risk sexual behavior. The CDC guidelines clearly address the need for health education as part of follow-up. In college health, we are usually fortunate enough to have health promotion experts on our staff We have made a health promotion visit a required part of our PrEP clinic follow-ups. Most specialists don’t . . .
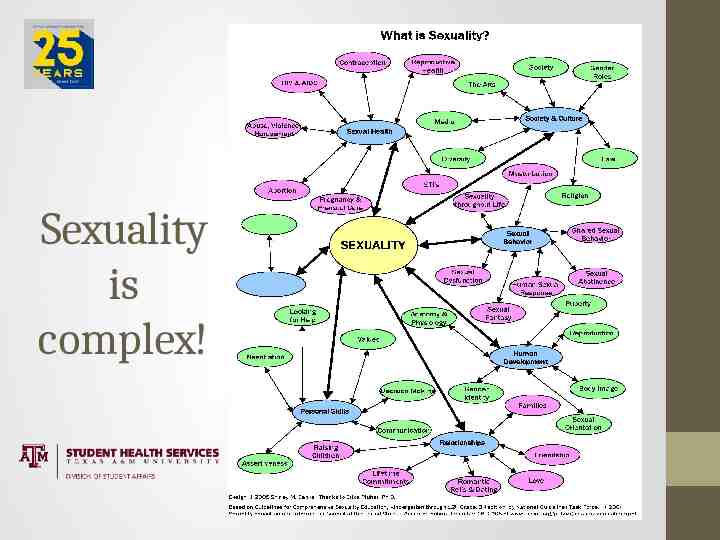
Sexuality is complex!
Tips from our Emory Sexual Health Educators A good way to ask about sexual identity and sexual behavior: “What genders do you have sex with?” Remember that patients often want to talk about sexual issues, but wait and watch for signs that their provider is open to such a discussion. It is your responsibility to take the lead. Take the initiative by routinely including questions about sexuality in your patient encounters. You might consider amending your Review of Systems to include a section on sexuality.
Tips from our Emory Sexual Health Educators (2) Communicate in plain, everyday language. Avoid the use of jargon. Exhibit a nonjudgmental attitude through your responses and questions. Never phrase a question so that a negative answer is the easiest response. Instead of “Have you ever . . . ,” try “When was the last time . . .” or “How often . . . .” Be prepared for some embarrassment or awkwardness, but don’t allow it to be a deterrent.
Tips from our Emory Sexual Health Educators (3) Reward and encourage patient initiative by saying “I’m glad you brought up this important issue.” Keep the door open for further discussion. Say “Let’s talk about this more next time,” or “This is an essential topic to revisit in the future; let’s agree to bring it up again.” Practice, practice, practice having these discussions with most of your patients until sexuality becomes a routine topic.
Discussion Topic #3 Attendees pair up into twos and discuss the following: You are the Student Health Services Director at a small liberal arts college. You started providing PrEP treatment (including a health promotion focus) at your center 2 months ago. In your one-on-one meeting today with your Student Affairs Vice President, she tells you that she is receiving concerned feedback from parents and faculty that PrEP promotes promiscuity among MSM students, reduces condom use, and will likely increase STI rates among students. How might you respond?
3. Work with your ID experts At EUSHCS, we do not believe that PrEP is a primary care medication . . . yet. Create an initial Memorandum of Understanding with your ID consultants to cover: Participation in the initial evaluation of students for suitability for PrEP Interpretation of initial lab results Initial prescribing of medication At least one follow-up visit to assess compliance and side effects Coordinated transfer of care to SHS/Primary Care Ease of access to consultation if problems arise
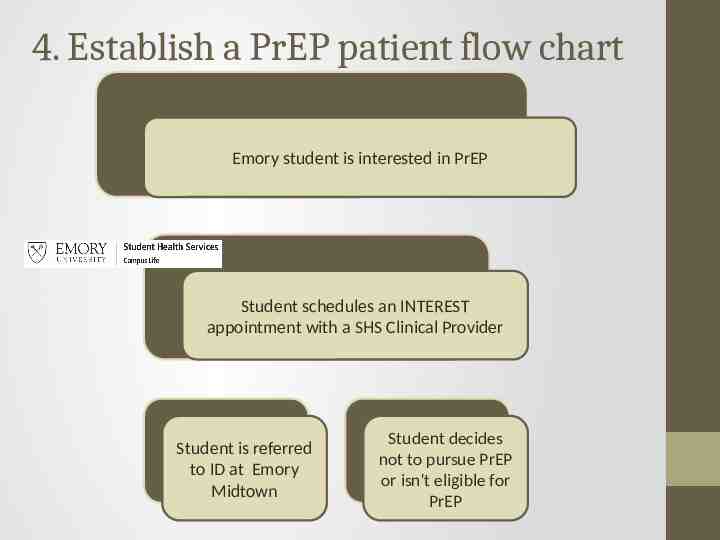
4. Establish a PrEP patient flow chart Emory student is interested in PrEP Student schedules an INTEREST appointment with a SHS Clinical Provider Student is referred to ID at Emory Midtown Student decides not to pursue PrEP or isn't eligible for PrEP
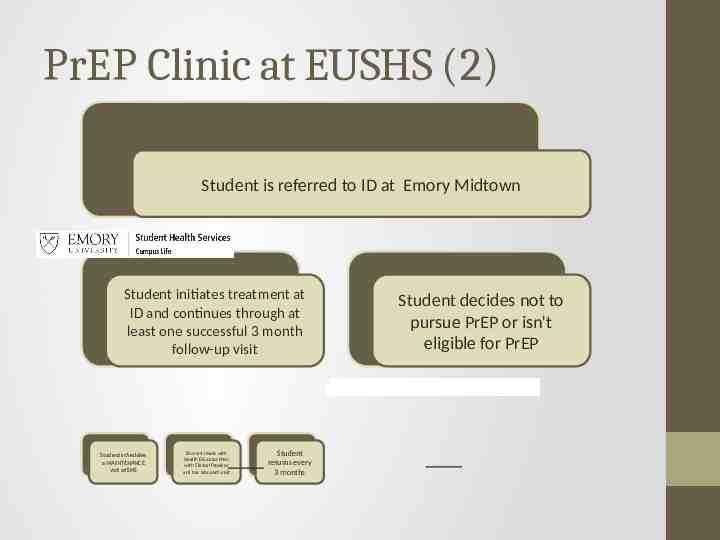
PrEP Clinic at EUSHS (2) Student is referred to ID at Emory Midtown Student initiates treatment at ID and continues through at least one successful 3 month follow-up visit Student schedules a MAINTENANCE visit at SHS Student meets with Health Educator then with Clinical Provider and has labs each visit Student returns every 3 months Student decides not to pursue PrEP or isn't eligible for PrEP
5. Create templates and handouts for the PrEP Clinic Emory University Student Health and Counseling Services Welcome to Your Patient Portal Items marked with **are required. PrEP (HIV Pre-Exposure Prophylaxis) Visit Instructions: Please complete this form prior to being seen for your appointment. For your Student Health Services PrEP Visit, you will meet with the Health Educator, have a medication management visit with your Clinical Provider, and have laboratory testing done. It is likely that the entire visit process with take 90 minutes, so please plan accordingly. PLEASE NOTE: THIS QUESTIONNAIRE WILL NOT BE READ BY A CLINICIAN UNTIL THE TIME OF YOUR VISIT. If you are experiencing chest pain, severe difficulty breathing, confusion, severe dizziness or other symptoms of acute distress, you should not schedule an appointment and instead call 911 or go to the nearest hospital emergency room. If you are unsure if you can wait to be seen at an appointment, please call 404-727-7551 and ask to speak to the nurse or the on call physician. ** Are you currently taking anti-retroviral medication (Truvada) to prevent HIV infection? Yes No ** If "yes," who prescribed it for you? An Emory Student Health Services provider Emory Infectious Diseases HIV Clinic at Midtown Other (please elaborate below) ** When was your most recent PrEP visit? Comments: ** Have you experienced any side effects of taking Truvada? Yes No Unsure If "Yes" or "Unsure," please elaborate: We have Point and Click templates for the Patient Portal questionnaire, PrEP Interest Screening Visit, PrEP Health Educator Visit, and PrEP Clinical Provider Follow-up Visit (and in 2017: PrEP Initial Clinical Provider Visit) CDC has excellent patient information handouts about PrEP
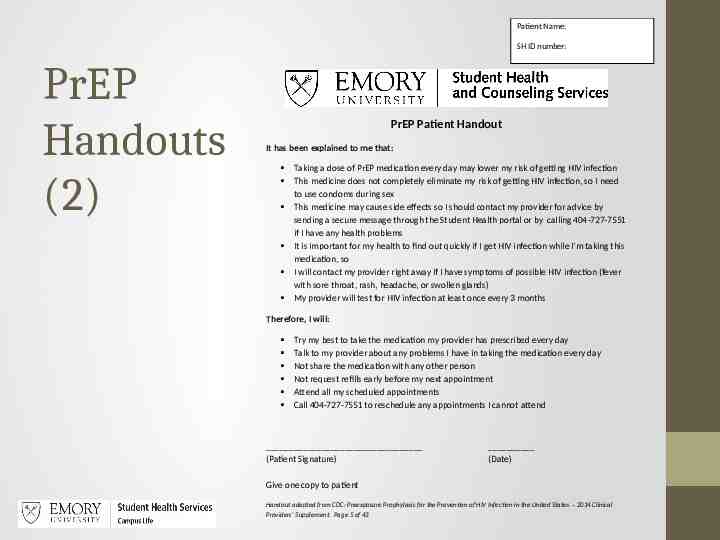
Patient Name: SH ID number: PrEP Handouts (2) PrEP Patient Handout It has been explained to me that: Taking a dose of PrEP medication every day may lower my risk of getting HIV infection This medicine does not completely eliminate my risk of getting HIV infection, so I need to use condoms during sex This medicine may cause side effects so I should contact my provider for advice by sending a secure message through the Student Health portal or by calling 404-727-7551 if I have any health problems It is important for my health to find out quickly if I get HIV infection while I’m taking this medication, so I will contact my provider right away if I have symptoms of possible HIV infection (fever with sore throat, rash, headache, or swollen glands) My provider will test for HIV infection at least once every 3 months Therefore, I will: Try my best to take the medication my provider has prescribed every day Talk to my provider about any problems I have in taking the medication every day Not share the medication with any other person Not request refills early before my next appointment Attend all my scheduled appointments Call 404-727-7551 to reschedule any appointments I cannot attend (Patient Signature) (Date) Give one copy to patient Handout adapted from CDC: Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2014 Clinical Providers’ Supplement. Page 5 of 43
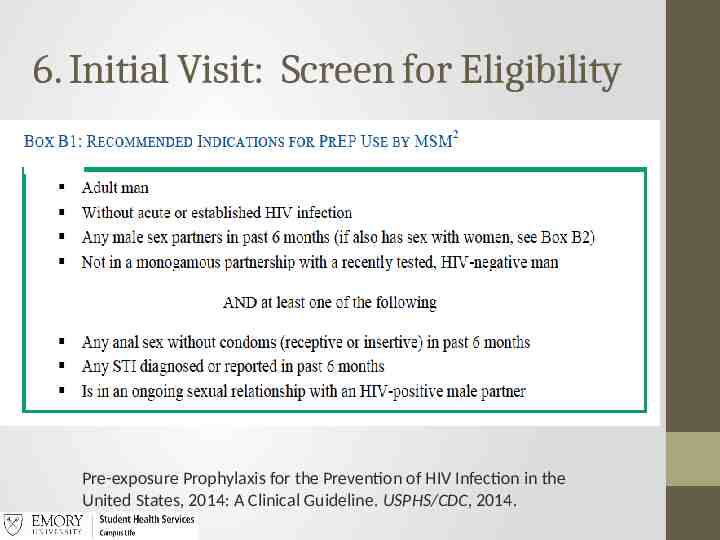
6. Initial Visit: Screen for Eligibility Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014.
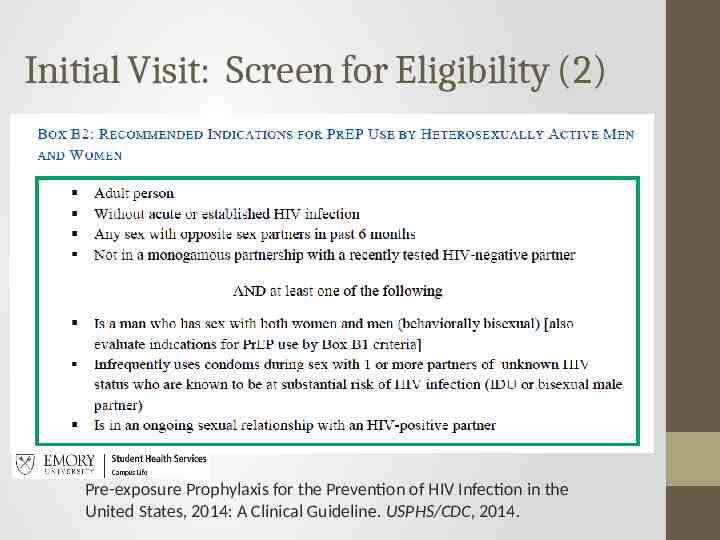
Initial Visit: Screen for Eligibility (2) Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014.
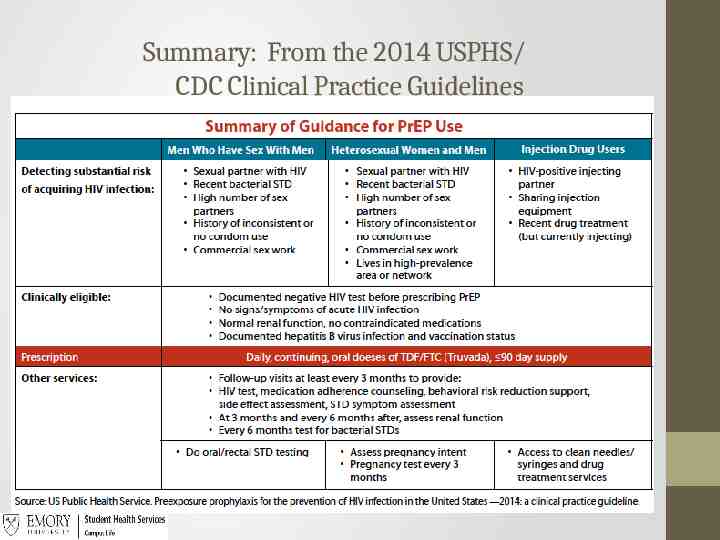
Summary: From the 2014 USPHS/ CDC Clinical Practice Guidelines
Knowledge Assessment #4 Which of the following is not considered a USPHS/CDC eligibility criteria for PrEP use in MSM? 1. Absence of acute or established HIV infection 2. Not in a monogamous relationship with a recently-tested HIV-negative man 3. Any anal sex without condoms (receptive only) in the past 6 months 4. Is in an ongoing sexual relationship with an HIV-positive partner
Knowledge Assessment #4 Which of the following is not considered a USPHS/CDC eligibility criteria for PrEP use in MSM? 1. Absence of acute or established HIV infection 2. Not in a monogamous relationship with a recently-tested HIV-negative man 3. Any anal sex without condoms (receptive only) in the past 6 months Receptive or Insertive 4. Is in an ongoing sexual relationship with an HIV-positive partner
7. PrEP Health Education Visit: Example of Risk Reduction and Adherence Question In the last 30 days, how many times have you missed taking a dose of your PrEP medication? Possible Probes if they say they have missed taking a dose at least once: On a scale of 0-10 how motivated are you in take a dose of your PrEP every day? How confident are you that you can take your PrEP medication every day? Additional probe: What would it take to get you to a higher 0-10 motivation number?
PrEP Health Education Visit: Example of MSM Risk Index Question Now I’m going to ask you the CDC’s specific questions for assessing HIV risk for men who have sex with men. In the last 6 months, with how many men have you had sex? Possible Probes for the above if they say more than 5: How interested are you on a scale of 0-10 in having fewer sexual partners? How confident are you that you can have fewer sexual partners? What would it take to get you to a higher number? What are some personal values or life goals that are most important to you? How does having fewer partners relate to those values and/or life goals?
Interactive Helpful Tool: CDC HIV Risk Estimator interactive tool https://wwwn.cdc.gov/hivrisk/estimator.html
8. TDF/FTC 2-drug combination: Tenofovir (TDF) and Emtricitabine (FTC) Mechanism of Action: Block important pathways that the virus uses to set up infection and therefore slows spread of HIV Emtricitabine: Nucleoside analogue of cytidine; inhibits activity of HIV-1 reverse transcriptase (RT) by competing with natural substrate deoxycytidine 5'-triphosphate and by being incorporated into nascent viral DNA, which results in chain termination. Tenofovir: Acyclic nucleoside phosphonate diester analogue of adenosine monophosphate; inhibits activity of HIV-1 RT by competing with the natural substrate deoxyadenosine 5'-triphosphate and, after incorporation into DNA, by DNA chain termination. One tablet daily Must use caution if kidney or liver disease ID consultant If you contract HIV and continue TDF/FTC, drug resistance can occur
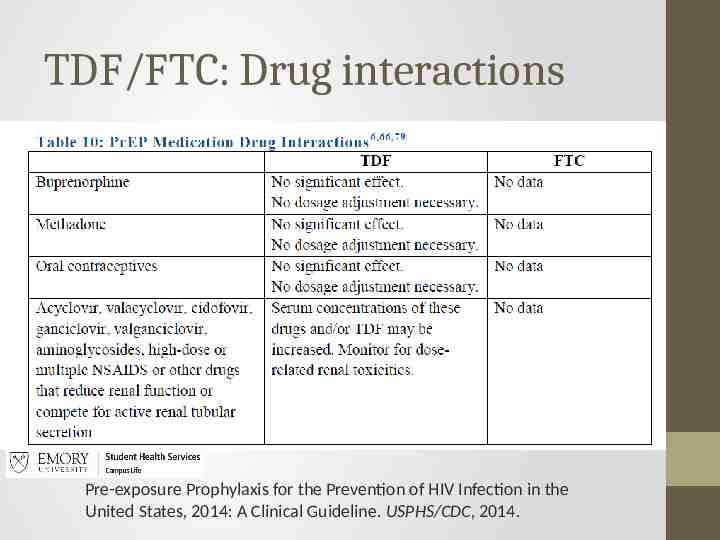
TDF/FTC: Drug interactions Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014.
TDF/TFC: Side effects Common: usually fade in one month Upset stomach Flatulence Headache Vomiting Loss of appetite “Contact your provider right away for” Fever or chills Especially with sore throat, cough, rash, myalgias, joint pains, diarrhea, malaise
TDF/FTC: Missed dose Take missed pill right away However, if almost time for next dose, then skip missed pill and take regular dose Do NOT take a double dose to make up for missed pill Missing doses impacts efficacy – this is not a “prn medication” PrEP is not PEP
Knowledge Assessment #5 Which of the following drugs presents potential drug interaction issues with TDF/FTC (choose all that apply)? 1. 2. 3. 4. Oral contraceptives Valacyclovir High dose NSAIDs Aminoglycosides
Knowledge Assessment #5 Which of the following drugs presents potential drug interaction issues with TDF/FTC (choose all that apply)? 1. 2. 3. 4. Oral contraceptives Valacyclovir High dose NSAIDs Aminoglycosides
9. 90-day Follow up Visits Patient informed when scheduling that the total visit (Health Promotion, Clinical Provider, Lab) will take 90-minutes Health Promotion: Assessment of medication adherence counseling support Assessment of HIV risk behavior counseling support (including condom use) Clinical Provider Assessment of HIV status, including signs/symptoms of acute HIV infection (Remember: symptoms usually last for 14 days after HIV exposure) Assessment of STI symptoms Assessment of medication side effects
Labs HIV testing every 3 months or sooner if symptoms of acute HIV Other STI testing (oral, anal, urethral) every 6 months or sooner if symptoms Renal function every 3 months initially, then every 6 months (eCrCl of 60 ml/min )
Medication Refill 90-day supply Truvada Follow up required in 3 months No refills given early, even if lost/misplaced (or shared) Medication handout given Signature of patient
10. Does a PrEP Clinic work at a College Health Service? Yes, it does . . .If you build it, they will come Emory Student Health: 2015 - 13 visits by 12 patients 12 PrEP Interest 1 PrEP Follow-up Emory Student Health: 2016 - 64 visits by 39 patients 31 PrEP Interest 33 PrEP Follow-up But even so: PrEP 0.48% of Primary Care visits and 0.30% of all clinical visits in 2016
Emory Student Insurance Plan PrEP TDF/FTC (Truvada) went from off the list (2013-14) to #5 (2014-15) to #1 (2015-16) most costly drug for the Emory Student Insurance Plan (FYI, estimated date for Truvada to go generic is 2021) Lots of other universities are in the PrEP biz!
Knowledge Assessment #6 Which of the following is a contraindication to continuing TDF/FTC Rx (choose all that apply)? 1. A positive HIV test result 2. Symptoms of acute HIV infection 3. Repeatedly positive STI testing (RPR, GC, Chlamydia) at 3-6 month testing 4. A creatinine clearance (eCrCl) 60 ml/min 5. Upset stomach and flatulence
Knowledge Assessment #6 Which of the following is a contraindication to continuing TDF/FTC Rx (choose all that apply)? 1. A positive HIV test result 2. Symptoms of acute HIV infection 3. Repeatedly positive STI testing (RPR, GC, chlamydia) at 3-6 month testing 4. A creatinine clearance (eCrCl) 60 ml/min 5. Upset stomach and flatulence
11. Are we increasing STIs in our MSM students with PrEP? (2) Our EUSHS primary care clinicians have expressed alarm at an apparent increase in STIs in our MSM students on PrEP, including a patient with permanent hearing damage from neurosyphilis. HIV Plus Study: Regular use of PrEP may reduce bacterial sexually transmitted infections; February 16, 2017 A joint study by the Centers for Disease Control and Prevention and the Rollins School of Public Health at Emory University suggests there is a significant reduction in the transmission of not only HIV, but other STIs for those who are using PrEP and receiving regular STI screenings and treatment.
11. Are we increasing STIs in our MSM students with PrEP? (2) Bay Area Reporter February 22, 2017 Researchers at Rollins School of Public Health determined that chlamydia infections would fall by 40 percent and gonorrhea infections by 42 percent over the next decade in the U.S. if 40 percent of PrEP-eligible men who have sex with men started taking the once-a-day pill of Truvada and were tested for STDs biannually. "Clinicians have a critical role to perform the recommended STI screening and treatment, as incidence could increase if PrEP is delivered without those services," wrote lead author Samuel Jenness, Ph.D., an assistant professor of epidemiology at Emory.
One possible next step. . . CDC (Atlanta and Kenya), Emory School of Public Health and Emory Student Health Services (!?!) are collaborating on a study to create and measure the efficacy of a contraceptive ring that also contains anti-retrovirals. Primary focus is likely to be in Sub-Saharan Africa in HIVdiscordant couples. Will this approach prove effective at both contraception and HIV prophylaxis? Will women be less likely to “miss doses” of PrEP anti-retrovirals if they are eluted from a contraceptive ring? They seem like questions worth asking.
Take Home Messages PrEP is effective. PrEP is expensive. PrEP prevents HIV, but not Chlamydia, GC, Syphilis, HSV, etc. With a thoughtful and careful approach, appropriate infectious diseases consultant backup (but not necessarily involvement), and adequate primary care and health promotion capabilities, HIV PrEP medication can be managed in many college health settings.
References 1. Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: A Clinical Guideline. USPHS/CDC, 2014. 2. Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States, 2014: Clinical Provider Supplement, USPHS/CDC, 2014. 3. Baeten JM, Donnell D, Ndase P, et al., Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. New England Journal of Medicine. 2012;367(5):399-410. 4. Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587-2599 5. Sullivan, PS et. al., Understanding Racial HIV/STI Disparities in Black and White Men Who Have Sex with Men: A Multilevel Approach, PLoS One 2014 Mar 7;9(3):e90514.
Questions? Michael J. Huey, MD Emory University Student Health Services [email protected] Sterling LaBoo Texas A&M University [email protected]