Meeting our returning combat veterans in the classroom Jonathan R.






























34 Slides168.81 KB
Meeting our returning combat veterans in the classroom Jonathan R. Sills, Ph.D. VA Palo Alto Health Care System December 2, 2010 [email protected]
Objectives Expand understanding of diagnostic signs symptoms of Mild Traumatic Brain Injury and Post Traumatic Stress Disorder. Share some ways that educators can work more effectively with those students who display mixed mTBI/PTSD symptoms Sills (2010)
Traumatic Brain Injury (TBI) is often identified as the signature injury of the recent conflicts.
DoD Health Affairs Workgroup TBI Definition A traumatically induced structural injury and/or physiological disruption of brain function as a result of an external force. (Vanderploeg 2008) Sills (2010)
TBI is an event that result in one or more of the following 1. Any period of loss or decreased level of consciousness 2. Any loss of memory for events immediately before or after the injury 3. Any alteration in mental state at the time of the injury (e.g., confusion, disorientation, slowed thinking) 4. Neurological deficits (e.g., weakness, balance disturbance, praxis, paresis/plegia, change in vision, other sensory alterations, aphasia.) that may or may not be transient 5. Sills (2010) Intracranial abnormalities (e.g. contusions, diffuse
Causes of TBI: Civilian and Military Civilian Populations Motor Vehicle Accidents (MVA) Sports Injuries Falls Gun Shot Wounds Military Populations Same as Civilian Explosions/Blast Injuries Pressure wave, shrapnel/debris, coup/contrecoup, crush Sills (2010)
Disruptions in cognitive functioning often associated with TBI Impairments in Attention Slowed Information Processing Learning/Memory Impairments Difficulties In Abstract Reasoning Diminished Executive Functioning (Sequencing, Planning, Initiation and Inhibition of Behaviors) Sills (2010)
Recovery of Cognitive Functions Cognitive functioning generally improves with natural healing and with cognitive retraining. Pace of cognitive return is variable based on intensity of injury– Mild, Moderate, Severe. Returns in attentional deficits usually occur prior to any returns in Executive Functioning or Delayed Memory. Mild and Moderate post injury baseline will generally be achieved within 1 to 2 years. Sills (2010)
Uncertainty of outcome during the recovery process contributes to distress which along with TBI ,may contribute to functional impairments in Cognitive, Behavioral, or Emotional functioning.
How do helpers (Health Care Providers, Educators, Family Members) respond to distress? Attempt to apply their skills to the best of their ability and often use methods that they have confidence in. Example –Psychologists may conduct Psychological Assessment. Results in of Multi Axial Diagnoses Initiation of treatment interventions based on diagnosis Sills (2010)
Three Major Sources of Data Clinical History Mental Status Exam Conclusion/ Diagnosis Sills (2010) Test Data
What’s in a Mental Status Exam? Judgment Orientation Insight Memory Affect/Appearance Thought (content & process) Sills (2010)
Assessment Difficulties TBI usually results in behavior and emotional changes that can mimic other psychiatric disorders. Developing a clear diagnostic impression is complicated. Sills (2010)
Behavioral and Emotional changes often associated with TBI Increased irritability Increased impulsivity Increased apathy More easily agitated Increased aggression Depression Anxiety Socially Inappropriate (DVA 2003; Vanderploeg 2006) Sills (2010)
Psychological or Organic Etiologies (DVA 2003) Psychogenic/Psychatric Symptoms Neurogenic Symptoms Denial Anosognosia (lack of awareness of impairment) Anger and irritability Frustration, catastrophic reaction. Depression Lack of initiative, fatigue, impaired Limited Emotional Expression Compulsive/hypervigilance Preservation, Failure to multitask Dependence on external controls Emotional lability Lability of emotional expressiveness. Social withdrawal Lack of initiative. Limited sense of the future Impaired planning Thought disorder Aphasia, anomia, or confusion Personality or conduct disorder Impulsivity, social disinhibition Sills (2010)
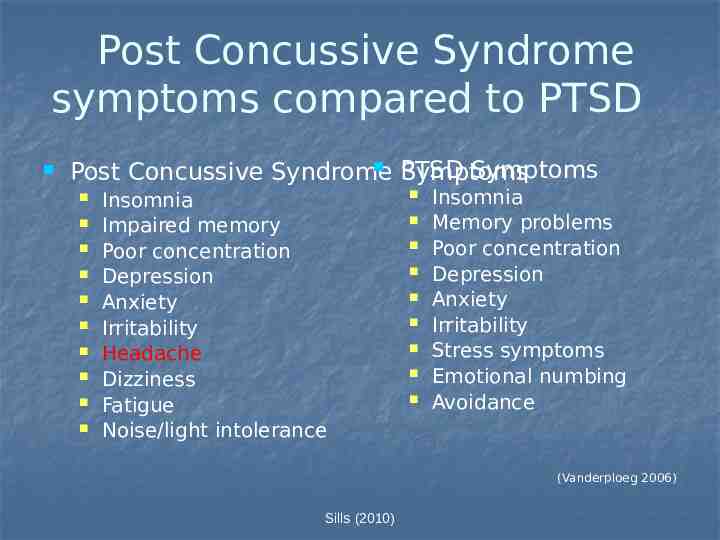
Post Concussive Syndrome symptoms compared to PTSD PTSD Symptoms Post Concussive Syndrome Symptoms Insomnia Impaired memory Poor concentration Depression Anxiety Irritability Headache Dizziness Fatigue Noise/light intolerance Insomnia Memory problems Poor concentration Depression Anxiety Irritability Stress symptoms Emotional numbing Avoidance (Vanderploeg 2006) Sills (2010)
Differential Diagnosis between Post-Concussion Syndrome & PTSD PTSD symptoms include reexperiencing of the trauma or numbing of general responsiveness, while PCS does not. PCS is characterized by headaches, dizziness, ringing in ears, generalized memory problems, or subjective intellectual impairment, while PTSD is not. (Mittenberg and Strauman 2000 from DVA 2003) Sills (2010)
Comorbity in Mild TBI Populations RAND Corporation Study (2008) Surveyed 1,965 service members 18.5% met criteria for either PTSD or depression 19.5% reported a probable mild TBI 37.4% of those individuals with a history of mTBI also had either PTSD or depression (Vanderploeg 2008) Sills (2010)
Complex Comorbid Relationship between PTSD and SUD PTSD and substance abuse co-occur at a relatively high rate Estimates of substance use disorders and PTSD Rate among patients in SUD treatment ranges from 12%-59% 58% of veterans in SUD programs have lifetime PTSD 73% of male Vietnam veterans who met diagnostic criteria for PTSD also qualified for lifetime SUD disorders (Walser 2008) Sills (2010)
25% of Returnees Report Problematic Drinking After Deployment (Hoge, 2004; Walser 2008) Pre-Deployment 0.4 0.35 0.3 0.25 0.2 0.15 0.1 0.05 0 Army Afghanistan Army Iraq Marine Iraq 35% 29% 25% 24% 18% 17% 21% 13% Have you used alcohol more than you meant to? Sills (2010) Have you felt you wanted or needed to cut down on your drinking?
Diagnostic Picture is Complicated Example-Axis I: Cognitive Disorder NOS PTSD Major Depressive Disorder Polysubstance Abuse Axis II: Deferred R/O Personality Disorder NOS, cluster B traits Axis III: Reported Multiple TBI, Chronic Pain--Back Axis IV: Disruption in occupational, academic, and social functioning Sills (2010) Axis V: GAF 52
What to Do with this Clinical Presentation? (Uomoto 2008) Marital Stress Vocational/ Academic Financial Challenges PTSD Depression Stress Substance Abuse Disorder Limitations in Role Functioning And Participation Blast Exposure TBI Impairment in Function and Social Reintegration Possible Diagnosis Sills (2010)
Theories of PTSD Biological Responses to Danger Flight, Fight, or Freeze Existential– Violation of “What is Right” Themis– a mark of civilized existence, sometimes it means right custom, proper procedure, social order, or justice. (Shay 1994 and 2003) Sills (2010)
Tips for working with students Educate yourself about military culture. Example -- Active Duty vs. Reserve Sills (2010)
Active Duty vs. Reserve Active duty currently serving full time in military. Military reserve force citizens who combine a military role or career with a civilian career. Reservists during cold war performed minimum of 39 days of military duty a year. In support of the Global War on Terror, a large number of Reservists have been performing in operational capacity for an extended period of time. Reservists tend to be older than active duty service members Sills (2010)
How educators can support learning for this population Educators Should Slow Down Remember TBI makes the world appear to be moving at a higher rate of speed than pre injury. Be More Directive in Office Hours Manage Expectations for Success Accommodate for Current Cognitive Functioning. Play to students cognitive strengths Sills (2010)
Ways to Play to Cognitive Strengths Use Mnemonics Provide Cues and “Chunking” of Information Use Stories Provides context and aids with recall of information Use repetition minimize confusion distributed practice effect Use Visual Aids Provide information across multiple sense modalities Sills (2010)
Various experiences of working with student’s that display an mTBI/PTSD symptoms May display a tendency to view things in all or nothing manner. May display a tendency to focus on perceived threats. Negative Intrusive Thoughts and Existential Issues can contribute to communication breakdowns Sills (2010)
Tips for working with students with mTBI/PTSD Provide control and decision making when possible Paper vs Midterm Group Projects inside vs outside of class Support cognitive flexibility by asking questions that allow for 3 points of view. Be mindful of location of seating Be mindful of making ad hoc statements that add minimal value to learning and can be easily misconstrued. Sills (2010)
“Learning Opportunities”-- Classroom Examples Clinical Psychology Applied Cultural Anthropology Talking about human behavior, disorders, and diagnosis without a warning introduction Environmental scanning and community mapping activities outside of class Philosophy and Political Science class Discussions Example -- Platonic dialogue “Laches” (Courage) which begins with two fathers discussing if their sons should be trained to fight in armor. Sills (2010)
Educators should “Holdfast.” Humble – check your ego. Observe – the student and your feelings. Listen – to what the student is telling you. Dedication – be available. Fair– Don’t expand things out of proportion or make excuses that end up unnecessarily lowering expectations. Athentic— Don’t lie, exaggerate, get competitive (male staff in particular) or pretend to be something that you are not. Stay with principles -- Be clear on your priorities and act accordingly. Truthworthy – Be consistent. Testing over time trust. Sills (2010)
In Review Combat veterans are returning from the current conflicts with a variety of comorbid conditions and challenges. Educators can support learning in returning combat veteran students by expanding their own knowledge of these conditions, military culture, and by making minimal changes to their established teaching practices. Sills (2010)
Thank You Questions? Sills (2010)
References Collins, R. (2006) Polytrauma Rehabilitation: A New Model of Care. Paper presented at the VA Psychology Leadership Conference held in Dallas Texas. Department of Veterans Affairs (2003) Traumatic Brain Injury: Independent Study Course. Veterans Health Initiative Kennedy, M (2008) Family Centered Care within Interdisciplinary Polytrauma Rehabilitation, Paper presented at the VA National Polytrauma Conference held in San Diego, California. Neibuhr, S (2008) Professional Self Care: protecting and sustaining your vitality, effectiveness and resilience?, Paper presented at the VA National Polytrauma Conference held in San Diego, California. Ruzek,J (2008) Towards PTSD treatment improvement for Veterans, National Center for PTSD Clinical training program Shay, J. (1994) Achilles in Vietnam: Combat trauma and the undoing of character. New York: Scribner Book Company Shay, J. (2003). Odysseus in America: Combat Trauma and the Trials of Homecoming. New York: Scribner Book Company. Uomoto, J (2008) VA outpatient Care for PTSD and Mild TBI/Polytrauma, Paper presented at the VA National Polytrauma Conference held in San Diego, California. Vanderploeg, R. (2008) Mild TBI and Mental Health Comprbidities: What do we Know?, Paper presented at the VA National Polytrauma Conference held in San Diego, California. Vanderploeg, R. (2006) Traumatic Brain Injury within the VHA and DoD Systems of Health Care, Paper presented at the VA Psychology Leadership Conference held in Dallas Texas. Wasler, R (2008) Posttraumatic stress disorder and Substance Abuse: Dual Diagnosis overview and Treatment, National Center for PTSD Clinical Training Program Zeiner, H. (2007) War Stories from Ward 7-D. California Connected. Programming aired Sills Television (2010) on KQED Bay Area Public Access Network. For more information see