Late and End of Life Topics: The Basics Jamie Capasso, DO































39 Slides2.09 MB
Late and End of Life Topics: The Basics Jamie Capasso, DO Geriatric Fellow UCI Program in Geriatrics
Topics Covered: After this presentation students . Will have a brief historical perspective in end of life medicine Will have an introduction in techniques of discussion of end of life topics with patients Will be comfortable with Decision-making ability; capacity vs. competency Can differentiate between Advanced directives vs. Living will vs. POLST Be familiar with the terms Power of attorney vs. Surrogate decision-maker
Topics Covered: After this presentation, students . Will be familiar with Hospice: Philosophy, benefits offered, common diagnoses and indicators Will have an introduction to Palliative Care Will know common myths and legality of Physician-assisted suicide
1565- Physicians tending to a dying patient
Historical Perspective In 1835, Jacob Bigelow urged fellow members of the Massachusetts Medical Society to withhold "therapies,” such as cathartics and emetics, from hopelessly ill patients. In 1848, John Warren, the surgeon who performed the first operation with ether anesthesia, urged that ether should be used "in mitigating the agonies of death.“ In 1953, John Bonica published the first textbook of pain medicine, suggesting a change in how opioids could be used for chronic pain. During the same time period, Dr. Cicely Saunders began work with terminal cancer patients and established the first hospice at St. Christopher’s in London in 1967.
Historical Perspective Parallel developments were occurring in many countries, and the first US hospice was established in New Haven, CT in 1974. From there, hospice grew exponentially. 1982 marked hospice being named as an entitlement by the Federal Medicare program. 1991: Patient Self-Determination Act- Hospitals required to inform patients of their rights including: The right to accept or refuse treatment The right to have an advanced directive The right to facilitate their health care decisions
Topics Covered: Will have a brief historical perspective in end of life medicine Will have an introduction in techniques of discussion of end of life topics with patients Will be comfortable with Decision-making ability; capacity vs. competency Can differentiate between Advanced directives vs. Living will vs. POLST Be familiar with the terms Power of attorney vs. Surrogate decision-maker
End of Life Discussion “Hope for the best, but prepare for the worst.” Allow equal time for hoping and preparing This facilitates discussion of a broad range of topics pertaining to future planning. Align patient and physician hopes Hope is an important coping mechanism and gives patients and their families gratification.
End of Life Discussion “Hope for the best, but prepare for the worst.” Encourage, but do not impose, the dual agenda of hoping and preparing. Don’t block/ignore such feelings as fear, anger, sadness or anxiety. Unarticulated fears are correlated to increased anxiety and depression. Name and discuss them. Support the evolution of hope and preparation over time. Probe: If reluctant to discuss these matters, Why?
Time your discussion early in the illness and revisit the issues regularly. Respond to emotions Communication strategies such as acknowledgement, exploration, legitimation, and empathy.
Topics Covered: Will have a brief historical perspective in end of life medicine Will have an introduction in techniques of discussion of end of life topics with patients Will be comfortable with Decision-making ability; capacity vs. competency Can differentiate between Advanced directives vs. Living will vs. POLST Be familiar with the terms Power of attorney vs. Surrogate decision-maker
Competence vs. Capacity Competence defines a legal status. A person is legally either competent or incompetent, with no gray areas in between. An adult is assumed to be competent unless he or she is determined by a court to lack the ability to make the decisions required for living safely, at which time the court deems that person incompetent.
Competence vs. Capacity Decision-making capacity implies the ability to understand the nature and consequences of different options, to make a choice among those options, and to communicate that choice. Decision-making capacity is thus required in order to give informed consent. When applied to medical decisions, this requires that a person understand a diagnostic or therapeutic intervention's significant benefits, risks, and alternatives
Topics Covered: Will have a brief historical perspective in end of life medicine Will have an introduction in techniques of discussion of end of life topics with patients Will be comfortable with Decision-making ability; capacity vs. competency Can differentiate between Advanced directives vs. Living will vs. POLST Be familiar with the terms Power of attorney vs. Surrogate decision-maker
Advance Directives Include three parts: 1. Living will AKA Health care directives: Legal document that spells out which medical treatments/life sustaining measures you do and do not want. 2. Medical Power of Attorney AKA Durable Power of Attorney for Health Care: designates an individual (proxy) to make medical decisions on your behalf if you are unable.
Advance Directives 3. DNR or Code status designation
Advance Directives MPOA goes into effect only when a patient is deemed incapacitated by illness. These documents do not require a lawyer- most only require two witnesses or a notary signature depending on the state. Some do not transfer state to state; have a patient that resides in two states complete two different forms. Go to caringinfo.org for state-specific form
Advance Directives Some state’s AD allows you to also designate a primary physician. Medicare reimburses for one “Advanced care planning” visit per 5 years, or additional visits when there is a major change in condition. Ensure that the patient has a discussion with the appointed proxy and physician regarding clear wishes for their future treatment.
POLST Physician orders for life-sustaining treatment Turns treatment wishes of an individual into actionable medical orders. Designed to be portable between facilities. Supplements the Advance Directive. Differs in that the POLST contains medical orders for current treatment, whereas the AD contains instructions for future treatments. Adopted by 9 states so far, mostly on the east and west coasts. There are 14 additional states developing programs.
Hierarchy of Surrogates Advance directives specified by the patient before (s)he became incapacitated prevail, even over the contrary wishes of guardians and other surrogate decision-maker. Family members and friends take precedence next, usually in the following order: Spouse Adult children Siblings Other family members Friend Health care providers follow, in the absence of other decisionmakers (not optimal)
We have a long way to go . Less than 50 percent of the severely or terminally ill patients studied had an advance directive in their medical record. Only 12 percent of patients with an advance directive had received input from their physician in its development. Between 65 and 76 percent of physicians whose patients had an advance directive were not aware that it existed. Advance directives helped make end-of-life decisions in less than half of the cases where a directive existed. Advance directives usually were not applicable until the patient became incapacitated and "absolutely, hopelessly ill." Providers and patient surrogates had difficulty knowing when to stop treatment and often waited until the patient had crossed a threshold over to actively dying before the advance directive was invoked. Language in advance directives was usually too nonspecific and general to provide clear instruction.
Topics covered . Students will be familiar with Hospice: Philosophy, benefits offered, common diagnoses and indicators Will have an introduction to Palliative Care Will know the basics of Physician-assisted suicide
Question: An 86 y/o woman is hospitalized for symptoms of abdominal pain, poor appetite, and progressive weight loss. Medical history of CAD and DM. Her physical functioning has declined: She can only walk a few steps and is dependent in all ADLs except feeding. CT of the abdomen and chest strongly suggest metastatic pancreatic cancer. She has undergone many procedures and hospitalizations and she doesn’t want anymore. She and her daughter inquire about hospice. Which of the following services is covered under the Medicare Hospice Benefit? A. Room and board in a long-term care facility B. Nursing care in a post acute-care nursing facility C. Hospital bed and bedside commode for home D. Private-duty caregiver at home E. Medications for diabetes and CAD
Patients with Medicare part A are eligible for the Medicare hospice benefit if they have a terminal illness with a life expectancy of 6 months or less. The benefit covers a variety of services related to the terminal diagnosis, including the provision of DME (hospital bed, bedside commode.) It also covers home-health aides, homemaker services, nursing visits, physician visits, social services, counseling, physical therapy, occupational therapy. It covers medications for comfort and palliation, but not for non-terminal conditions (the DM and CAD.)
Hospice In general, designed to shift the focus of care from curative to comfort in a person nearing the end of life. Relies on physician assertion that if a patient follows the normal course of their disease, their life span will be less than 6 months. Philosophy centered in multidisciplinary care, focusing on maximizing the quality of life, not necessarily the quantity.
Team Members Physician Nurses Home health aid Social Worker Chaplain Volunteers
Common Hospice Diagnoses Cancer: failed or decline treatment Heart failure: frequent hospitalizations, poor symptom control on max medicines AIDS Hepatic failure/Cirrhosis
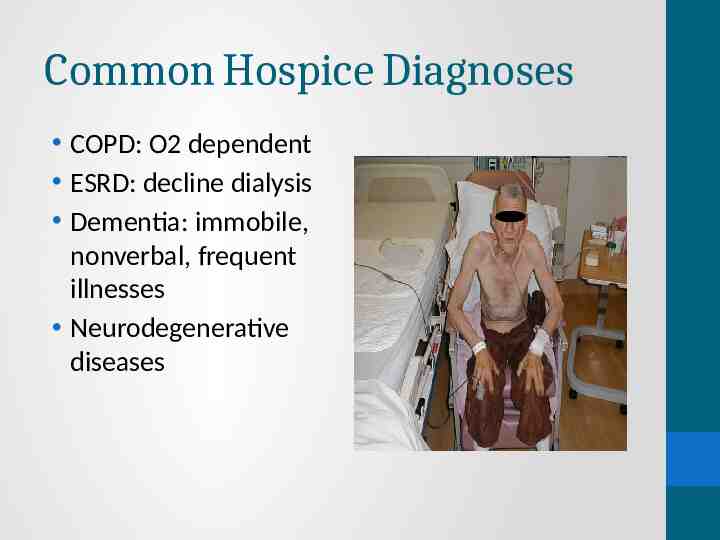
Common Hospice Diagnoses COPD: O2 dependent ESRD: decline dialysis Dementia: immobile, nonverbal, frequent illnesses Neurodegenerative diseases
Topics covered . Students will be familiar with Hospice: Philosophy, benefits offered, common diagnoses and indicators Students will have an introduction to Palliative Care Will know the basics of Physician-assisted suicide
Palliative Care Focus on symptom management, can complement Hospice care, but can also be used while pursuing curative treatments. Symptoms of: Pain Dyspnea Depression Anxiety Swelling Nausea, GI distress
Palliative Care Can use modalities such as: Medicines Counseling Acupuncture PT Procedures Pet therapy
Topics covered . Students will be familiar with Hospice: Philosophy, benefits offered, common diagnoses and indicators Will have an introduction to Palliative Care Will know the basics of Physician-assisted suicide
Physician-assisted Suicide Only legal in Netherlands, Belgium, and Switzerland. Oregon, Montana, and Washington in the US have also legalized the practice. It consists of offering a patient a prescription, medication, information, or other intervention with the understanding that the patient intends to use them to commit suicide. The term euthanasia is different: it implies active voluntary euthanasia- this is when the physician actively intervenes to end the life of a patient with their consent. “Passive,” or “indirect“ euthanasia refers to the practice of removal of life-sustaining treatments such as ventilation or artificial feeding. These practices are not euthanasia, and considered legal and ethical.
Physician Assisted Suicide Palliative care often involves the administration of powerful drugs including narcotics and benzodiazepines. These drugs may hasten death in some cases. The difference is intent: in these cases, the intent is to alleviate symptoms, not to end life. If a patient expresses a desire to seek PAS, start by having a conversation to inquire what their motivation is. Then, consider consultation with a palliative care specialist, or conduct a comprehensive assessment of the patient’s physical, psychological, social, and spiritual suffering. Address these issues with a multidisciplinary approach.
Questions?
References Hanks, Geoffrey W. C. Oxford Textbook of Palliative Medicine. Oxford: Oxford UP, 2010. Print. "Law for Older Americans." American Bar Association. Web. 05 Apr. 2011. http://www.americanbar.org/groups/public education/resou rces/law issues for consumers/ patient self determination act.html Kass-Bartelmes, Barbara L. "Advance Care Planning: Preferences for Care at the End of Life. "Agency for Healthcare Research and Quality (AHRQ) Home. Web. 08 Apr. 2011. http://www.ahrq.gov/research/endliferia/endria.htm
References "Frequently Asked Questions about Physicians Orders for LifeSustaining Treatment Paradigm (POLST)." OHSU Home. Web. 08 Apr. 2011. http:// www.ohsu.edu/polst/patients-families/faqs.htm Verdugo Hospice Care Center Los Angeles. Web. 08 Apr. 2011. http://www.verdugohospice.com/hospice circle.php "Download Your State's Advance Directives - CARING CONNECTIONS - NHPCO." Home - CARING CONNECTIONS NHPCO. Web. 30 Apr. 2011. http://www.caringinfo.org/i4a/pages/index.cfm?pageid 3289
References Applebaum P, Grisso T. Assessing patients' capacities to consent to treatment, N Engl J Med 1988;319:1635-1638. "AMDA: Governance - Resolutions and Position Statements White Paper on Surrogate Decision-Making and Advance Care Planning in Long-Term Care." American Medical Directors Association. Web. 14 Apr. 2011. http:// www.amda.com/governance/whitepapers/surrogate/index.cf m Emmanuel, Ezekiel J. "Euthanasia and Physician Assisted Suicide." Up to Date. 3 Jan. 2011. Web. 20 Apr. 2011
References Mas, Joan M. Communication. Illustration. 29 September 2007. Online image. Flickr. 1 April 2011. http://www.flickr.com/photos/dailypic/1459055735/ Copyright (c) a href 'http://www.123rf.com' 123RF Stock Photos /a Image ID: 8058801 Clip art courtesy of Microsoft