TWELVE STEP FACILITATION 2017 Joseph Nowinski, Ph.D.




72 Slides1.59 MB
TWELVE STEP FACILITATION 2017 Joseph Nowinski, Ph.D.
Source for Research Cited Nowinski, J. If You Work It, It Works! The Science Behind 12 Step Recovery, Center City, MN: Hazelden, 2015.
THE FORCE AWAKENS
STANTON PEELE, PH.D. “AA is Ruining the World” Here is why AA is harmful and will hurt societies: AA denies reality (There is no such thing as “addiction”) AA overemphasizes its own success AA rules out other, often more effective, approaches AA’s underlying temperance message actually creates alcoholism and addiction
Lance Dodes, M.D. “AA has the worst success rate in all of medicine.”
Most Common Complaints about AA: AA promotes powerlessness AA doesn’t work: other treatments are more effective AA exaggerates the need for abstinence AA is a religion and brainwashes its members. AA does not address the underlying causes of substance abuse. AA is a modern temperance movement. AA social status network: those who slip are stigmatized.
Does AA Promote Powerlessness? James Fowler, Ph.D. (d) Professor of Theology and Human Development, Emory University Stages of Spiritual Development “AA presents individuals with a paradoxical opportunity: By admitting powerlessness over alcohol they can become empowered through turning to others finding a spiritual belief system they can embrace”
Is AA a Social Hierarchy? 12 Steps: Traditional View
Is AA a Social Hierarchy? 12 Steps: Traditional View
12 Steps: Native American View
AA as a “Spiritual” Fellowship versus a Religion AA does advocate for “spiritual” values and activities. Humility (Step 1) Honesty (Moral Inventory) Community (Fellowship, Community Service, Volunteerism) Altruism (Step 12) Prayer & Meditation Spiritual Awakening/Epiphany (Steps 1-3, Step 12)
The “Underlying Causes” of Addiction Psychodynamic View (Lance Dodes et. al.) “I’ve found that addictive acts serve as a way to restore a sense of power when a person feels helpless.” Psychoanalytic Perspective All behaviors are symptomatic of underlying conflict. Powerlessness Addiction “Recovery” comes through long-term psychotherapy. No clinical trials. 12 Step View “We admitted that we were powerless over alcohol, that our lives had become unmanageable.” Perspective of those caught in the web of addiction: Addiction is the problem. Addiction Powerlessness. Recovery comes through sobriety and spiritual renewal. Recovery leads to empowerment.
Is AA is a Modern Temperance Movement? What is “temperance” and how does AA relate to it? Does AA and/or the treatment industry overplay addiction? Are harm reduction and controlled use viable alternative treatment goals? When is abstinence the appropriate treatment goal?
“The Drinking/Using Spectrum”
THE COMPETITION Alternatives to the AA 12 step model: Moderation Management and Harm Reduction (MM)
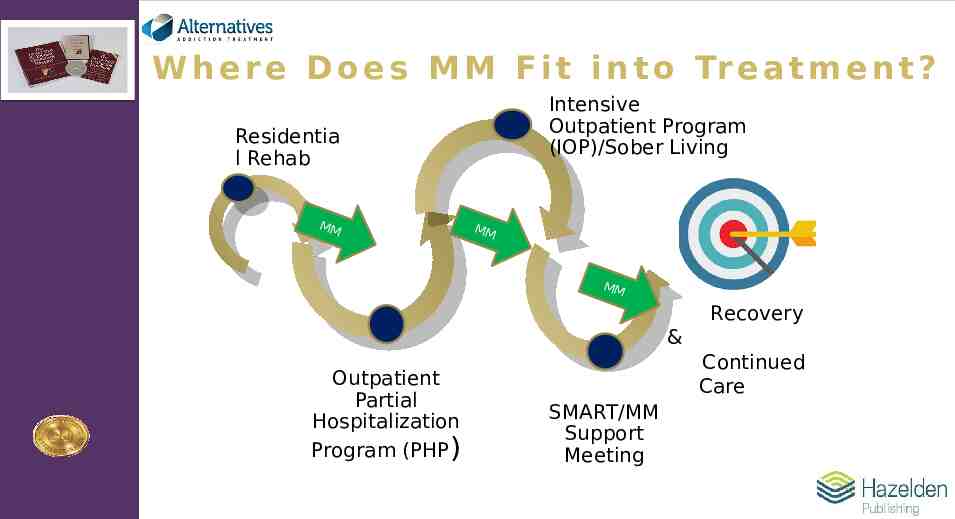
W h e r e D o e s M M F i t i n t o Tr e a t m e n t ? Intensive Outpatient Program (IOP)/Sober Living Residentia l Rehab MM MM MM MM Recovery & Outpatient Partial Hospitalization Program (PHP) Continued Care SMART/MM Support Meeting
Is AA a Social Hierarchy? 12 Steps: Traditional View
“Moderation Management” Humphreys (2001, 2003) Compared self-identified MM vs AA members. Problem severity significantly less among MM members. MM members more likely to be women, less than 35 years old. MM members more highly educated, employed full-time, and have family supportive of moderation. 15% of MM members self-reported blackouts, tremors, morning craving, and/or work/family problems in the prior 6 months. Only 3% of this 15% later opted for abstinence.
“Behavioral Self-Control Training” Miller et. al. (1992) BCS Goal Controlled Drinking. Manual-guided treatment: Goal Setting; Self-Monitoring; Self-Reinforcement; Identify High-Risk Situations & Alternatives to Drinking. N 140 (45%) men & women assessed 3, 5, 7, & 8 years post-treatment. Results: 23 voluntarily abstained; 14 reported non-problem drinking; 22 “impaired”; 35 “unremitted”; 46 unaccounted for. 14/94 14% success rate for this group
The Tyranny of “Abstinence-Only” The Center for Optimal Living Abstinence is only acceptable goal Commitment to abstain often a requirement of treatment Achieving abstinence quickly is often required Based on Jellinek’s Disease Model Pervades our culture www.centerforoptimalliving.com
The “Abstinence-only” Approach The Center for Optimal Living Split between addiction treatment and mental health treatment Informs an abstinence-only substance use treatment system Many mental health clinicians won’t treat active substance users Keeps people from seeking help 70% of public sector behavioral health patients in US diagnosed with co-occurring disorders Not supported by evidence www.centerforoptimalliving.com
What is Harm Reduction? PHILOSOPHY Shifts from abstinence-only to any reduction in drug-related harm or related issues without abstinence requirement Safer use, reduced use, moderation and abstinence fall under the harm reduction umbrella “Compassionate pragmatism” (Marlatt) “Come as you are” (Little) The Center for Optimal Living www.centerforoptimalliving.com
Abstinence vs. Controlled Drinking and “Conditional Abstinence” Bujarski et al (2013) N 1,226 (428 women) recruited from 11 treatment sites. Self-Identified Goal Options: Controlled Drinking; Total Abstinence; Conditional Abstinence. Treatment up to 20 sessions using predominantly CBT MET. Results: Those men and women who chose abstinence as their goal had the best outcome after treatment. Those with a goal of “controlled drinking” had the worst drinking outcomes. Finally, those who selected “conditional abstinence” had outcomes in between the two other groups.
For Whom is Abstinence an Appropriate Treatment Goal? Moderate/severe to severe substance use per DSM-5 (Moderate to Severe on the Drinking/Using Spectrum) Lack of social support for moderation Poor personal history with moderation Consequences (past & prospective)
Twelve Step Facilitation (TSF) No controlled research on the efficacy of AA prior to 1989. Institute of Medicine white paper (1989) made possible the development of Twelve Step Facilitation (TSF) for inclusion in Project MATCH and subsequent clinical trials. Additional research on “active ingredients” of 12 Step recovery followed on Project MATCH outcome.
Twelve Step Facilitation TSF a manual-guided intervention (“psychotherapy-assisted recovery”) based on the 12 Step model of recovery. TSF allows for individualized treatment planning. TSF is a comprehensive treatment that deals with 3 “dimensions” of recovery: Cognitive; Social/Behavioral; and Spiritual. TSF incorporates key 12 Step concepts along with cognitive-behavioral and motivational strategies
Project MATCH Largest psychotherapy outcome study ever conducted, compared: Cognitive-Behavioral Therapy (CBT) Motivational Enhancement Therapy (MET) Twelve-Step Facilitation (TSF)
Project Match Research Group Journal of Mental Health, 1998 “The three treatments had favorable effects on drinking and related outcome measures. The treatment effects endured over time periods from 12 months to 3 years.” Outcomes measures: Total abstinence Per cent days abstinent (PDA) Drinks per drinking day (DDD)
Project MATCH: 3-Year Outcome Longabaugh et. al. (1998) TSF and MET more effective than CBT after 3 years TSF more effective than MET for individuals whose social environments supported drinking Best predictor of outcome AA attendance
Wu & Wietkiewicz (2008) “For clients with social networks supportive of drinking, post-treatment drinking outcomes were significantly better if they were matched to TSF instead of CBT or MET.” “For those mismatched to CBT or MET network support for drinking was associated with greater accumulation of drinking consequences.”
John F. Kelly, Ph.D. “In Project MATCH it was found that TSF, as compared to CBT and MET, had more than double the number of patients who were continuously abstinent at one year after treatment, and about 1/3 more at the three year mark.”
William R. Miller, Ph.D. “On at least one time-honored outcome measure—the percentage of patients maintaining complete abstinence—those in the Twelve Step Facilitation treatment fared significantly better at all follow-up points than did patients in the other two conditions—a substantial advantage of about 10 percentage points that endured across three
Journal of Substance Abuse Treatment (2004) “Because longitudinal studies associate self-help group involvement with reduced substance use, improved psychosocial functioning, and lessened health care costs, there are humane and practical reasons to develop self-help group supportive policies.”
National Institute of Health “12-step treatments that facilitate engagement with AA post-discharge can not only produce about one third higher continuous abstinence rates, but also 64% lower health care costs compared to cognitive-behavioral treatments.”
U.S. Surgeon General Mutual aid groups and newly emerging recovery support programs and organizations are a key part of the system of continuing care for substance use disorders in the United States. A range of recovery support services have sprung up all over the United States, including in schools, health care systems, housing, and community settings. The state of the science is varied in the recovery field. Wellsupported scientific evidence demonstrates the effectiveness of 12-step mutual aid groups focused on alcohol and 12-step facilitation interventions. Source: addiction.surgeongeneral.gov/key-findings/recovery
TSF is “Evidence-Based” TSF has been evaluated via randomized clinical trials. Has undergone extensive blind peer review and has been selected for inclusion in National Registry of Evidence-based Programs and Practices (www.samhsa.gov/nrepp), as assessed via Comparative Evaluation Research (CER). American Psychological Association listing of “Empirically Supported Treatments” Approved for alcohol and drug abuse, and for individual or group treatment.
The End of Rehab? Several factors work against “rehab” as the future treatment of choice: Project MATCH outcome: no differences in outcome between aftercare and outpatient arms despite same initial diagnoses The emergence of community-based treatment plus medication-assisted recovery Cost (the rehab industry vs. third party payers) On-line resources Validation of evidence-based treatments such as TSF that are highly compatible with all of the above
TSF Handbook 2017 Second Edition Strong emphasis/guidelines for group administration as well as using TSF with adolescents Fewer/modified topics: “Moral Inventories” and “Relationships” dropped, conjoint program addresses “Family” approach, “Spirituality” added Streamlined session guidelines and fidelity checklists Includes TSF for Co-Occurring Disorders (TSFCOD) Expanded to apply to all Twelve Step recovery groups (not just AA and NA) Expanded emphasis on recovery dimensions to ensure balanced treatment plans Inclusive of participants in MAT programs Addresses common criticisms of Twelve Step fellowships DSM-5 Compliant
TSF: Treatment Goals Active involvement in a recovery fellowship (AA, NA, DTR, WFS) which advocates abstinence from alcohol and drug use and utilizes group support to help members stay sober. Relapse Prevention
TSFCOD: Treatment Goals Active involvement in a recovery fellowship plus active involvement in psychiatric treatment. Relapse Prevention
Longitudinal Studies Relevant to Relapse
Moos & Moos (2005) Followed 362 patients from pre-treatment to 1, 3, 8, and 16 years post-treatment who made voluntary choices: Group 1: Opted for AA with no other treatment Group 2: Opted for AA Concurrent treatment Group 3: Opted for treatment but not AA Results: Group 2 had greatest AA involvement and were most likely to remain clean and sober through 16 years People who dropped out of AA at any point were more likely to resume drinking
Witbrodt, Yu Ye, Weisner & Mertens (2014) 1,945 men & women who sought SUD treatment through the Kaiser Permanente system Required 1 AA or other 12 Step meeting/week during treatment only. AA, NA, etc. optional after that. Assessed 1, 5, 7 and 9 years post-treatment. Findings: Greater 12 step meeting attendance led to increases in 5-year abstinence and to a lesser extent in 7-year abstinence. Importantly our analysis extends findings to a diverse population of treatment seekers, namely men and women with alcohol and drug use disorders who were insured members of an integrated health care organization.
Sponsorship Witbroldt, et al. (2012): “Does Sponsorship Improve Outcomes Above Alcoholics Anonymous Attendance?” Assessed AA Attendance (low to high), Sponsorship (low to high), and Abstinence over a 7-year period. Results: Individuals in the high sponsorship group were 7 times more likely to remain abstinent than those in the low sponsorship group. Those men and women who maintained a sponsor over time had an added advantage over the group that no longer had a sponsor by year 7. Having an AA sponsor provided an advantage with respect to abstinence over and above meeting attendance alone.
Components of TSF Handbook: Used as a reference. Includes detailed descriptions of all TSF/TSFCOD topics, case examples, and discussions of research supportive of 12 step recovery as well as specific TSF content. Facilitator Guides: Provides succinct instructions for conducting TSF sessions individually or in groups, following the TSF structure. Session Fidelity Checklists: Designed to be used within TSF sessions as a convenient way for facilitators to follow the TSF treatment protocol. Can also be used to monitor TSF treatment adherence. Workbook: Contains complete exercises related to the TSF or TSF-COD program, and designed to be used during session facilitation and between sessions. Use reinforces participation and continued sobriety. Video: Briefly introduces each TSF topic. Assessment Tools: Include the TSAPS, which was developed by Audrey Klein, is within the public domain, and is reliable and valid
TSF Session Structure Step 1: REVIEW Follow-up on recovery tasks Participation Involvement (networking, sponsorship, etc.) Recognizing clean/sober days “Analyze” slips/relapses Reading
Analyzing Slips Step 1: Identify Context: Social: “Where Were You?” Cognitive: “What Were You Thinking?” Emotional: “What Were You Feeling?” Step 2: Identify Consequences Step 3: Create Alternative Scenarios
TSF Session Structure Step 2: NEW MATERIAL Core Program Elective Program Conjoint Program Termination
TSF Session Structure Step 3: RECOVERY TASKS Meetings Follow-up on new material Networking Readings Concurrent Mental Health Treatment (COD)
TSF Core Program CORE TOPICS Assessment Acceptance (Cognitive & Spiritual) Surrender (Cognitive & Spiritual) Getting Active (Social/Behavioral)
TSF Core Topic 2: Acceptance Use Session Checklist Follow TSF Structure: Review, New Material, Recovery Tasks
TSF Core Topic 2: Step 1: Acceptance Read Step 1 aloud and seek honest (gut) reactions, being open to denial or ambivalence Break down Step 1 and engage in discussion Solicit a “motivational rating” Identify “denial” and its forms as a natural response to loss of control Seek identification with forms of denial Define Step 1 as humility: acceptance of reality Solicit “acceptance rating”
TSF Core Topic 3: Steps 2 & 3: Surrender Use Session Checklist and follow TSF structure Step 1: Review Step 2: New Material Step 3: Recovery Tasks
TSF Topic 3: Surrender Read Step 2 aloud and seek honest reactions Discuss Step 2 in terms of hope (to overcome addiction) Who have patients turned to in the past in time of need? Solicit a “willingness rating”: accepting the idea that willpower alone is sometimes not enough to solve a problem Read Step 3 aloud and seek honest reactions Discuss Step 3 in terms of trust (in others for help and support) Solicit responses on what if any beliefs patients hold with respect to a “Higher Power” Who do patients trust for help in overcoming addiction?
Steps 1-3 and Epiphany “Epiphany” a moment when you suddenly feel that you understand, or suddenly become conscious of, something that is very important to you. “Spiritual Experience” (Alcoholics Anonymous): “Most of our experiences (epiphanies) are what the psychologist William James calls the ‘educational variety’ because they develop slowly over a period of time.”
TSF Elective Program Elective Topics: Genograms Enabling People, Places, and Routines (Social/Behavioral) Emotions Spirituality (Spiritual)
People, Places, & Routines
Litt et. al.- Changing Network Support for Drinking Compared three treatments for patients diagnosed with alcohol use disorders: Case Management: “Treatment as usual,” patients assigned to therapists who identified “barriers to recovery” to work on in treatment. Network Support: Based on TSF but included ANY non-drinking friends or family members in the revised support network. Network Support Plus Contingency Management: TSF plus random rewards for meeting attendance.
Litt et. al.-The Network Support Project (2009): 2-Year Follow-up 61% of those who received either the NS or its similar NS/CM treatment attended AA meetings regularly. In contrast, only 18% of those who received the Case Management (CM) treatment attended AA, and for this group the outcome was not as good. Patients who received Network Support (NS) treatment reported an average of 80% abstinent days 2 years after treatment had ended, and 40% were reporting complete abstinence in the 90 days preceding their 2-year follow-up. Adding even a single non-drinking friend to the social network helped, but not nearly as much as attending AA meetings. Participants in the NS/CM condition initially did as well as those in NS but at the end of 2 years were reporting the same outcomes as those in case management.
TSF Elective Topic: People, Places, & Routines Use Session Checklist Follow TSF Structure: Review New Material: The Lifestyle Contract Recovery Tasks
People, Places, & Routines “Resilient Recovery” NEW MATERIAL A “resilient” recovery a recovery that can withstand challenges. Lifestyle Contract relates to “getting active” and building a resilient recovery Three “pillars” of a resilient recovery: Belief: Steps 1, 2, & 3. Action: Involvement (Getting Active, People, Places, & Routines) Spirituality Explain the rationale: Creating and pursuing a Lifestyle Contract is a “blueprint” for building a resilient recovery
TSFCOD: Core Program Assessment Acceptance (Cognitive & Spiritual Dimension) Surrender (Cognitive & Spiritual Dimension) Getting Active in 12 Step Recovery (Social/Behavioral Dimension) Getting Active in Psychiatric Treatment (Social/Behavioral Dimension)
TSFCOD Elective Program ELECTIVE TOPICS Barriers to Getting Active in 12 Step Recovery Barriers to Getting Active in Psychiatric Treatment People, Places, and Routines Emotions Living for Recovery Enabling (in Conjoint Program)
TSF Elective Topic: Spirituality
Spirituality and Recovery Stephanie Carrol Spirituality and Purpose in Life in Alcoholism Recovery 100 AA members (51 male) Defined “spiritual” activities as prayer meditation reading spiritual material (Reading as a TSF Recovery Task) Communing with nature interacting with or creating art attending religious services engaging in AA service activities (community) volunteering to be a sponsor or temporary sponsor (altruism)
Spirituality and Purpose in Life in Alcoholism Recovery: Findings 50% reported daily prayer or meditation, plus listening to “spiritual” music at least weekly 50% reported reading spiritual material x3/week 50% reported interacting with art at least monthly 90% attended AA meetings at least twice a week
Spirituality and Recovery Kelly et. al. (2011): Spirituality in Recovery N 1,726. Assessed Spiritual Identity: Atheist: Not believing in God. Agnostic: Believing we can’t really know about God. Unsure: Doesn’t know what to believe about God. Spiritual: Believes in God but is not religious. Religious: Believes in God and practices a religion. Plus Spiritual Activities: Praying, Meditating, Attending Religious Services, Reading Holy or Spiritual Writings.
Kelly et. al.- Spirituality in Recovery Findings: Higher scores on spirituality/religiousness were positively related to PDA (abstinence) and negatively related to DDD (drinking). Men and women who reported stronger spiritual beliefs were more likely to remain abstinent, and to drink less if they did slip. Men and women in recovery showed significant increases in spiritual beliefs that was correlated with AA involvement, but Less than half attended formal religious services.
Spiritual Awakening: Fact or Fiction? At age 17 a troubled girl was admitted to a seclusion room at the Institute of Living in Hartford. Her behaviors included: burning her wrists with cigarettes; slashing her arms, her legs, and her midsection using any sharp object she could get her hands on; and banging her head on the floor. On discharge 26 months later she was described as one of the most disturbed patients in the hospital. “I was in hell.”
“Radical Acceptance” “One night, at age 20, I was kneeling and praying in the chapel in the Cenacle Retreat Center at Loyola University. “I was looking up at the cross and the whole place became gold—and suddenly I felt something coming toward me. It was this shimmering experience, and I just ran back to my room and said “I love myself. I felt transformed.”
Marsha Linehan, Ph.D., developer of Dialectical Behavior Therapy (DBT)
Thank You!