Bowel Obstruction Chapter 48: Ileus and Bowel Obstruction

39 Slides3.36 MB
Bowel Obstruction Chapter 48: Ileus and Bowel Obstruction
Bowel Obstruction True or False: A simple incomplete obstruction is defined by obstruction of blood to the segment of involved bowel leading to tissue necrosis and gangrene.
Bowel Obstruction Which of the following is considered a closed loop obstruction? 1.Intussusception 2.Bezoar 3.Diverticulitis 4.Volvulus
Bowel Obstruction 70% of the intraluminal gas within the intestine is? 1.Oxygen 2.CO2 3.Methane 4.Nitrogen
Bowel Obstruction The most common cause of small bowel obstruction is? 1.Malignancy 2.Adhesions 3.Meckel’s Diverticulum 4.Bezoar
Bowel Obstruction What is the bacterial count in normal feces? 1. 1 x 106 2. 1 x 109 3. 1 x 1010 4. 1 x 1011
Bowel Obstruction True or False: Laparoscopic exploration and lysis of adhesions is associated with a statistically significant decrease in post-operative complications, decreased time to return of bowel function, shortened length of stay, and decreased cost as compared to open exploration.
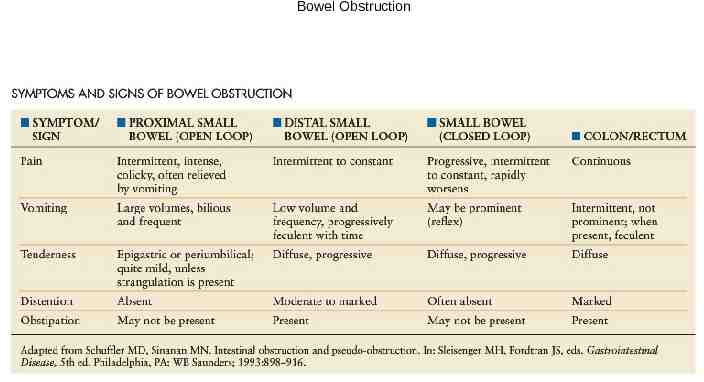
Bowel Obstruction Bowel Obstruction Inability of luminal contents to progress through the bowel – Mechanical Obstruction Incomplete vs. Complete Open vs. Closed Strangulation – Neurogenic/Functional Obstruction ileus
Bowel Obstruction
Bowel Obstruction Bowel Obstruction SBO: Etiology Adhesion #1 (80-90% of SBO in pt’s w/prior abdominal surgery) Hernia #2 overall - #1 cause of SBO in pts w/o prior abdominal surgery Tumor #3 LBO: Etiology Cancer #1,2,3
Bowel Obstruction Differential Age – Neonate: meconium ileus, Hirschsprung’s, malrotation, atresia – Child: intussusception, Hirschsprung’s – Adult: hernia, IBD, CA, diverticular disease – Elderly: CA, diverticular disease, Ogilvie’s
Bowel Obstruction
Bowel Obstruction PE Start with ABCs Look for surgical scars Bowel sounds Distension: distal obstruction proximal Localized tenderness: R/O peritonitis Look for hernias/masses Do a rectal exam
Bowel Obstruction Labs CBC: WBC (nml in uncomplicated SBO)/ Hb (anemia w/CA) BMP (hypoK, hypoCl) ABG: Alkalosis (a/w proximal obstruction)/ Acidosis (a/w bowel infarction) Amylase (may be elevated in SBO)
Bowel Obstruction Work-Up Obstructive series: look for free air, dilated bowel loops, air-fluid levels – Note: if cecal diameter 12cm, there is a risk of perforation. At 12-14cm, the wall tension perfusion pressure, increasing risk of necrosis CT scan Barium enema UGI series w/SB follow-through
Bowel Obstruction Management NPO – Bowel Rest Nasogastric Decompression IVF resuscitation Electrolyte Replacement /- Surgical Intervention
Bowel Obstruction Management
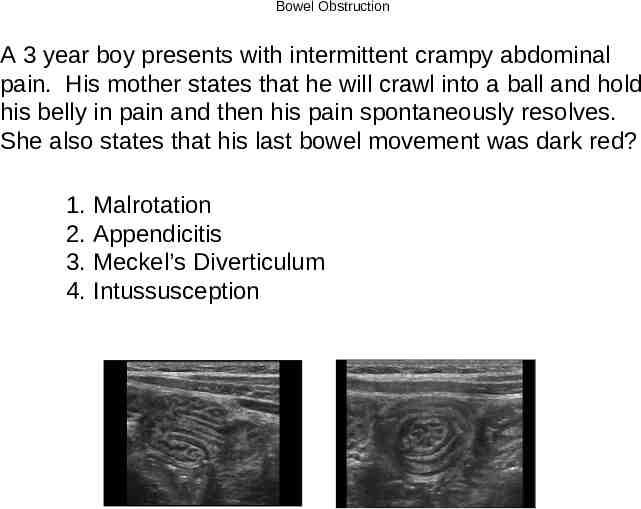
Bowel Obstruction A 3 year boy presents with intermittent crampy abdominal pain. His mother states that he will crawl into a ball and hold his belly in pain and then his pain spontaneously resolves. She also states that his last bowel movement was dark red? 1. Malrotation 2. Appendicitis 3. Meckel’s Diverticulum 4. Intussusception
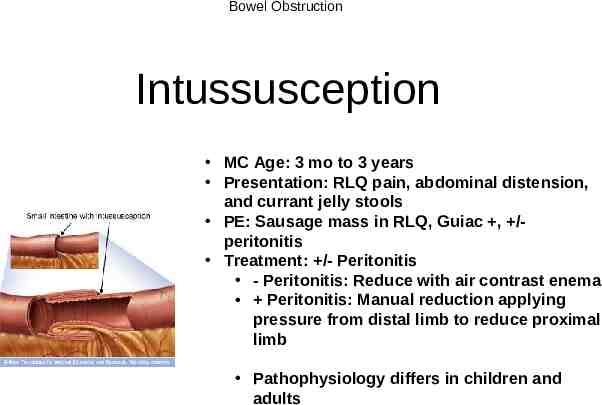
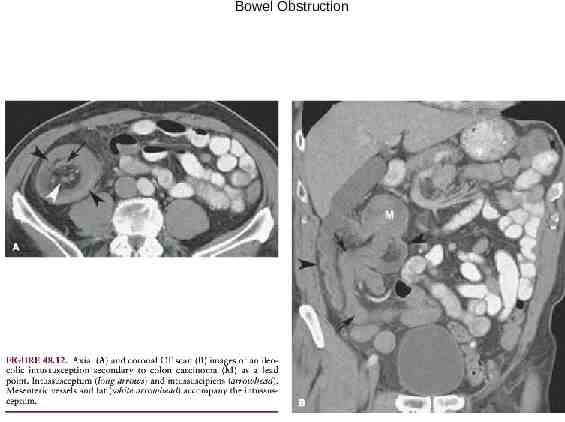
Bowel Obstruction Intussusception MC Age: 3 mo to 3 years Presentation: RLQ pain, abdominal distension, and currant jelly stools PE: Sausage mass in RLQ, Guiac , /peritonitis Treatment: /- Peritonitis - Peritonitis: Reduce with air contrast enema Peritonitis: Manual reduction applying pressure from distal limb to reduce proximal limb Pathophysiology differs in children and adults
Bowel Obstruction
Bowel Obstruction A 3 mo boy is brought to the emergency department with new onset bilious emesis. On exam he has no evidence of peritonitis or hemodynamic instability. The diagnostic test of choice is? 1. Obstructive series 2. CT abdomen/Pelvis 3. UGI 4. Abdominal US
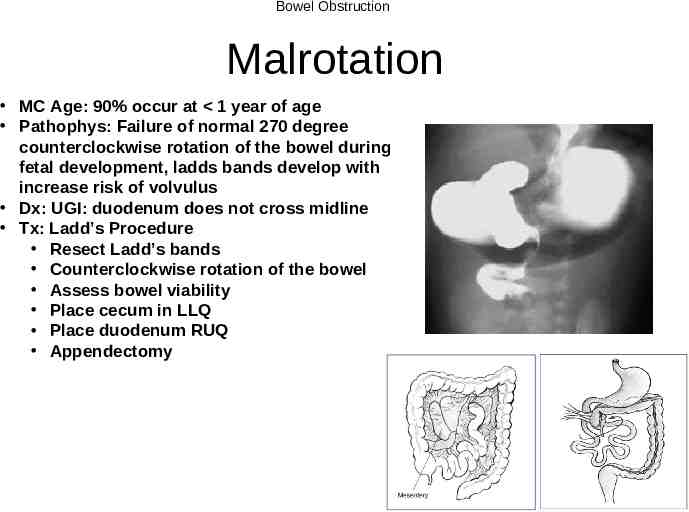
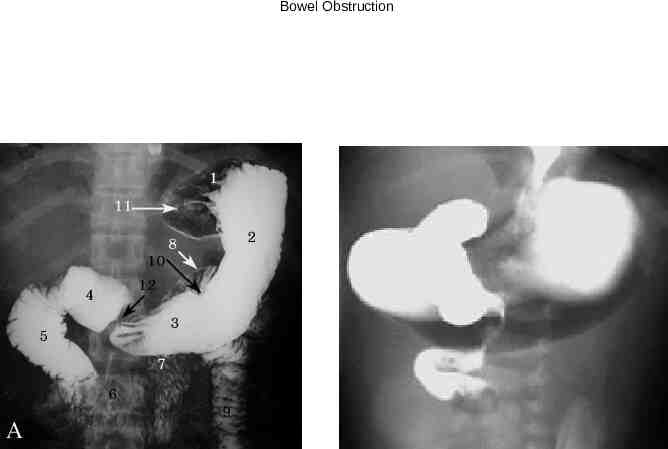
Bowel Obstruction Malrotation MC Age: 90% occur at 1 year of age Pathophys: Failure of normal 270 degree counterclockwise rotation of the bowel during fetal development, ladds bands develop with increase risk of volvulus Dx: UGI: duodenum does not cross midline Tx: Ladd’s Procedure Resect Ladd’s bands Counterclockwise rotation of the bowel Assess bowel viability Place cecum in LLQ Place duodenum RUQ Appendectomy
Bowel Obstruction
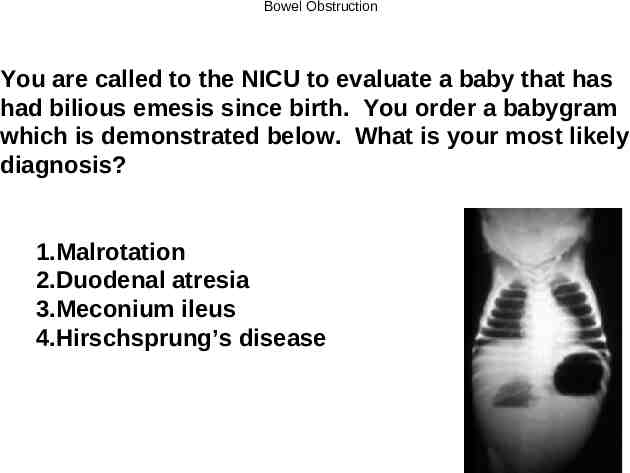
Bowel Obstruction You are called to the NICU to evaluate a baby that has had bilious emesis since birth. You order a babygram which is demonstrated below. What is your most likely diagnosis? 1.Malrotation 2.Duodenal atresia 3.Meconium ileus 4.Hirschsprung’s disease
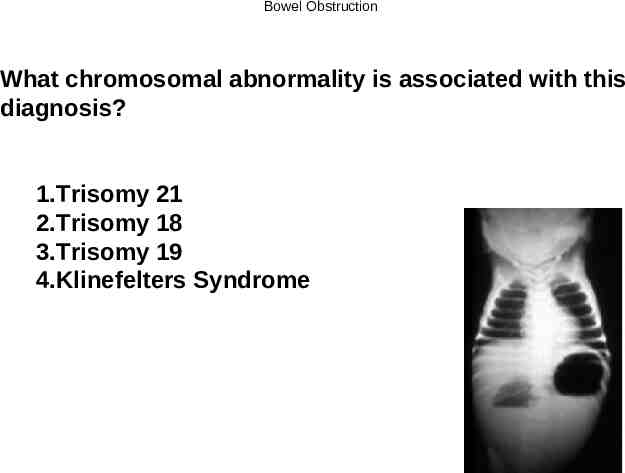
Bowel Obstruction What chromosomal abnormality is associated with this diagnosis? 1.Trisomy 21 2.Trisomy 18 3.Trisomy 19 4.Klinefelters Syndrome
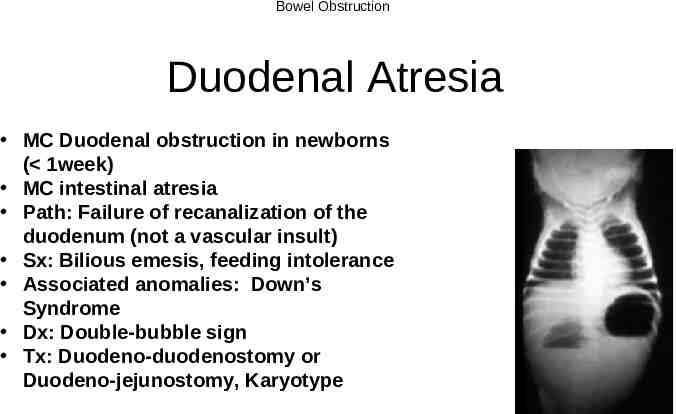
Bowel Obstruction Duodenal Atresia MC Duodenal obstruction in newborns ( 1week) MC intestinal atresia Path: Failure of recanalization of the duodenum (not a vascular insult) Sx: Bilious emesis, feeding intolerance Associated anomalies: Down’s Syndrome Dx: Double-bubble sign Tx: Duodeno-duodenostomy or Duodeno-jejunostomy, Karyotype
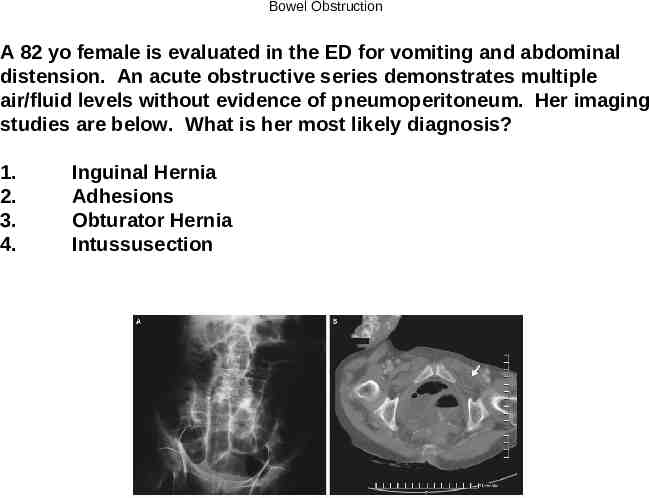
Bowel Obstruction A 82 yo female is evaluated in the ED for vomiting and abdominal distension. An acute obstructive series demonstrates multiple air/fluid levels without evidence of pneumoperitoneum. Her imaging studies are below. What is her most likely diagnosis? 1. 2. 3. 4. Inguinal Hernia Adhesions Obturator Hernia Intussusection
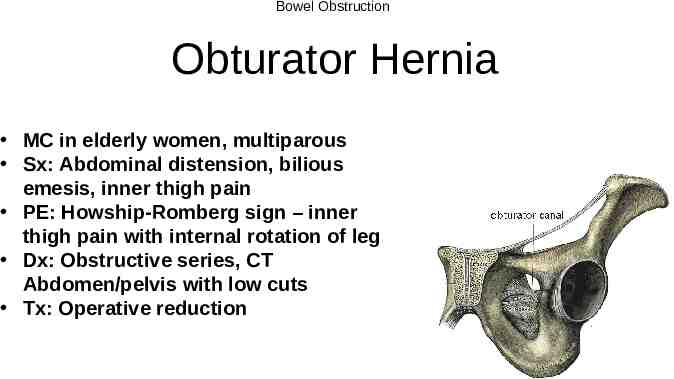
Bowel Obstruction Obturator Hernia MC in elderly women, multiparous Sx: Abdominal distension, bilious emesis, inner thigh pain PE: Howship-Romberg sign – inner thigh pain with internal rotation of leg Dx: Obstructive series, CT Abdomen/pelvis with low cuts Tx: Operative reduction
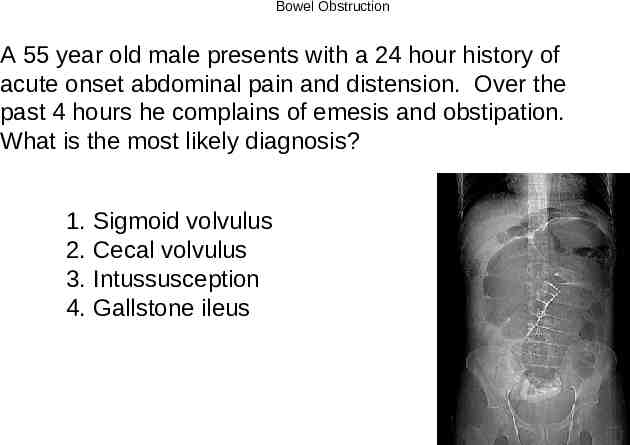
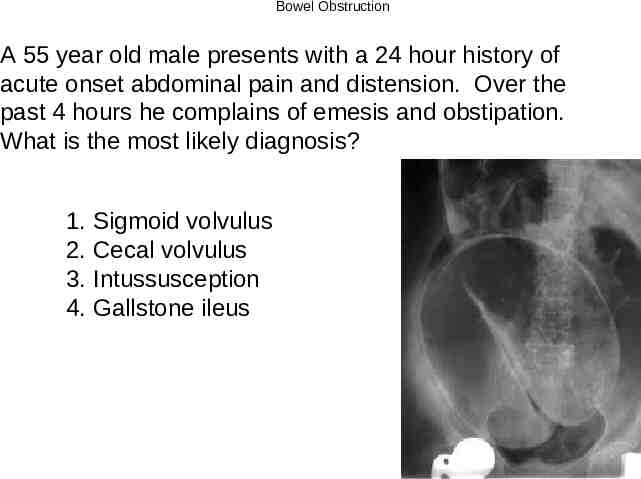
Bowel Obstruction A 55 year old male presents with a 24 hour history of acute onset abdominal pain and distension. Over the past 4 hours he complains of emesis and obstipation. What is the most likely diagnosis? 1. Sigmoid volvulus 2. Cecal volvulus 3. Intussusception 4. Gallstone ileus
Bowel Obstruction A 55 year old male presents with a 24 hour history of acute onset abdominal pain and distension. Over the past 4 hours he complains of emesis and obstipation. What is the most likely diagnosis? 1. Sigmoid volvulus 2. Cecal volvulus 3. Intussusception 4. Gallstone ileus
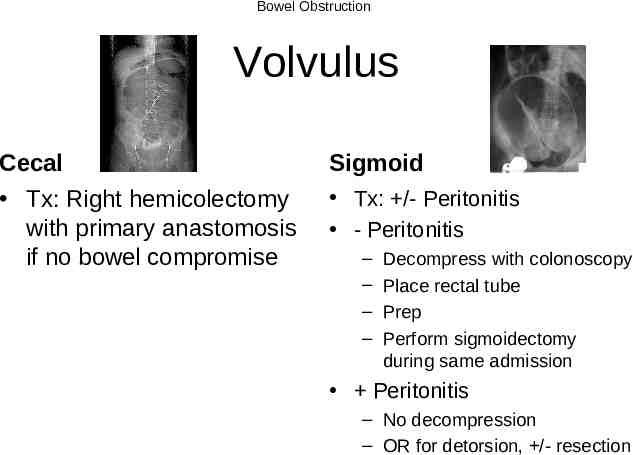
Bowel Obstruction Volvulus Cecal Tx: Right hemicolectomy with primary anastomosis if no bowel compromise Sigmoid Tx: /- Peritonitis - Peritonitis – – – – Decompress with colonoscopy Place rectal tube Prep Perform sigmoidectomy during same admission Peritonitis – No decompression – OR for detorsion, /- resection
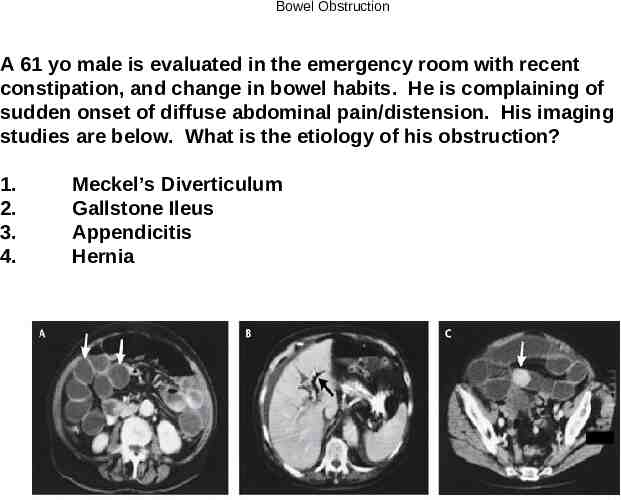
Bowel Obstruction A 61 yo male is evaluated in the emergency room with recent constipation, and change in bowel habits. He is complaining of sudden onset of diffuse abdominal pain/distension. His imaging studies are below. What is the etiology of his obstruction? 1. 2. 3. 4. Meckel’s Diverticulum Gallstone Ileus Appendicitis Hernia
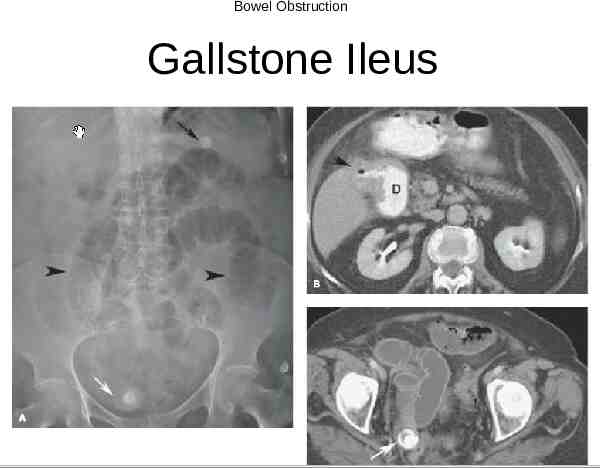
Bowel Obstruction Gallstone Ileus
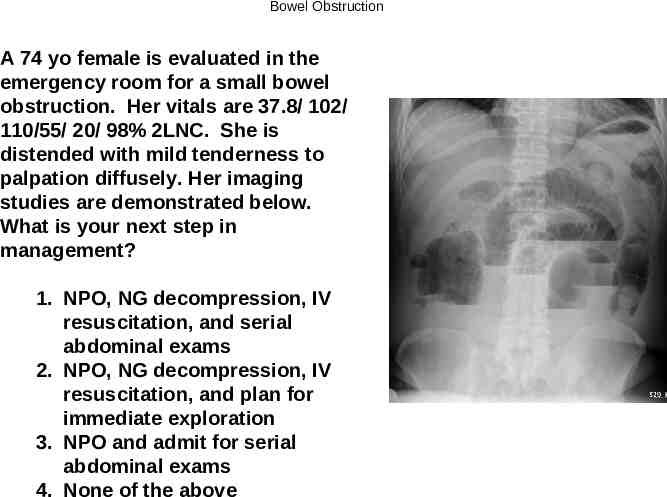
Bowel Obstruction A 74 yo female is evaluated in the emergency room for a small bowel obstruction. Her vitals are 37.8/ 102/ 110/55/ 20/ 98% 2LNC. She is distended with mild tenderness to palpation diffusely. Her imaging studies are demonstrated below. What is your next step in management? 1. NPO, NG decompression, IV resuscitation, and serial abdominal exams 2. NPO, NG decompression, IV resuscitation, and plan for immediate exploration 3. NPO and admit for serial abdominal exams 4. None of the above
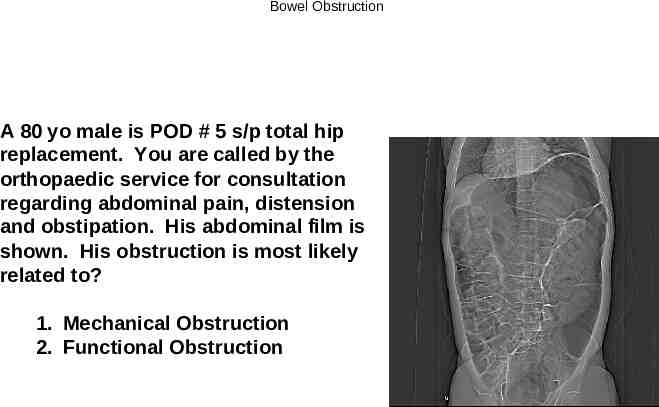
Bowel Obstruction A 80 yo male is POD # 5 s/p total hip replacement. You are called by the orthopaedic service for consultation regarding abdominal pain, distension and obstipation. His abdominal film is shown. His obstruction is most likely related to? 1. Mechanical Obstruction 2. Functional Obstruction
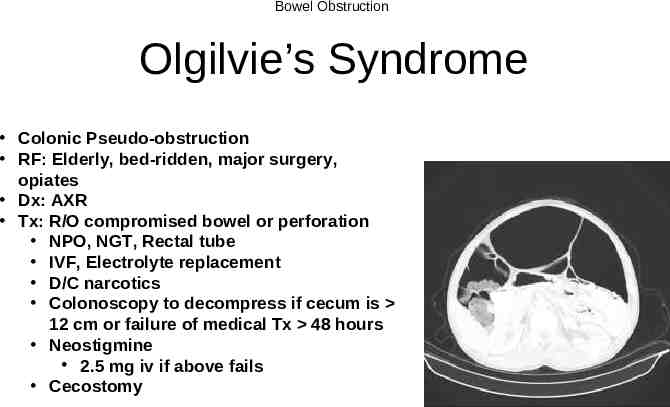
Bowel Obstruction Olgilvie’s Syndrome Colonic Pseudo-obstruction RF: Elderly, bed-ridden, major surgery, opiates Dx: AXR Tx: R/O compromised bowel or perforation NPO, NGT, Rectal tube IVF, Electrolyte replacement D/C narcotics Colonoscopy to decompress if cecum is 12 cm or failure of medical Tx 48 hours Neostigmine 2.5 mg iv if above fails Cecostomy
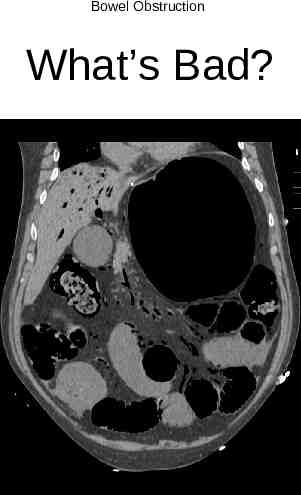
Bowel Obstruction What’s Bad?
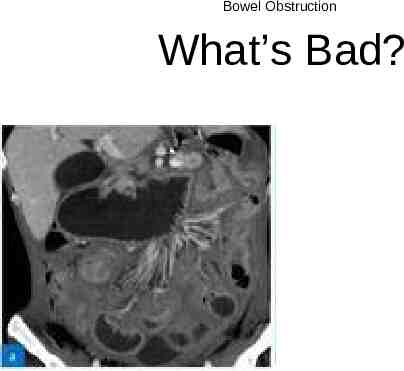
Bowel Obstruction What’s Bad?
Bowel Obstruction What’s Bad?