SAQ 27 – ANAESTHETICS / PROCEDURAL SEDATION Ben Cheung



19 Slides401.60 KB
SAQ 27 – ANAESTHETICS / PROCEDURAL SEDATION Ben Cheung
OVERVIEW 1. Disclaimer 2. SAQ 27 feedback - specific for each sub-question 3. Cohort analysis 4. Re-cap / general feedback 5. Questions / comments
1. DISCLAIMER Monash / Peninsula Health Pro Sat written FEx in 2018.1 – similar format can relate But was all handwritten for SAQs Con Not an ACEM examiner / in exam writing committee
2. SAQ 27 FEEDBACK Question on ”anaesthetics” Procedural sedation / ketamine 18 marks 5 sections / sub-questions Unexpected change to sub-question D and E More generous with marking of these sections Overall pass mark lowered
2. SAQ 27 FEEDBACK Grace is a 6 year old girl, who has been brought in by her father after she inserted a small bead into her right nostril. She has no significant past history, and has no regular medications or allergies. Her vital signs are within normal limits for age. Grace is 20 kg in weight. Although “parent’s kiss” has failed to expel the nasal foreign body, the bead is visible and anterior enough for removal in ED. The child however is very anxious about the procedure.
2. SAQ 27 (A) You have discussed a trial of midazolam with the father, and have reassured Grace a “no needle” approach to this anxiolytic medication. How would you prescribe this midazolam (route and dose in mg), and when would you expect peak sedative effect from time of administration? (2 marks) Oral / buccal midazolam, 0.3-0.5mg/kg 10mg 15-20 min from administration to peak effect Accepting up to 30 minutes, based on unpredictable oral absorption personal experience Reference: https://www.rch.org.au/uploadedFiles/Main/Content/comfortkids/RCHProcedure%20-PSWA.Mas ter.10022017.pdf
2. SAQ 27 (A) You have discussed a trial of midazolam with the father, and have reassured Grace a “no needle” approach to this anxiolytic medication. How would you prescribe this midazolam (route and dose in mg), and when would you expect peak sedative effect from time of administration? (2 marks) Common mistakes Using INTRANASAL route 0 marks Controversial whether child is supposed to “sniff” Either way, risk of FB aspiration if using intranasal route Stating IV or IM Incorrect dosing Errors ranged from 1mg to 30mg Not stating dose in mg Requirement explicitly stated in question Weight of child also listed in stem
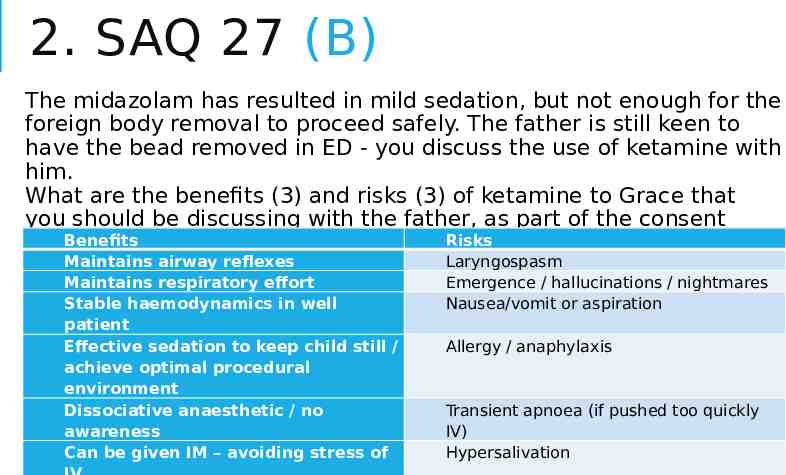
2. SAQ 27 (B) The midazolam has resulted in mild sedation, but not enough for the foreign body removal to proceed safely. The father is still keen to have the bead removed in ED - you discuss the use of ketamine with him. What are the benefits (3) and risks (3) of ketamine to Grace that you should be discussing with the father, as part of the consent Benefits Risks process? (6 marks) Maintains airway reflexes Maintains respiratory effort Stable haemodynamics in well patient Effective sedation to keep child still / achieve optimal procedural environment Dissociative anaesthetic / no awareness Can be given IM – avoiding stress of Laryngospasm Emergence / hallucinations / nightmares Nausea/vomit or aspiration Allergy / anaphylaxis Transient apnoea (if pushed too quickly IV) Hypersalivation
2. SAQ 27 (B) The midazolam has resulted in mild sedation, but not enough for the foreign body removal to proceed safely. The father is still keen to have the bead removed in ED - you discuss the use of ketamine with him. What are the benefits (3) and risks (3) of ketamine to Grace that you should be discussing with the father, as part of the consent process? (6 marks) Common mistakes Stating analgesic effect, without sedative effect ½ mark only Cannot assume layperson knows the effects of ketamine Analgesia also not the most important benefit of ketamine in this situation Parallels to use of BZD for agitation, and stating “able to abort seizure” as a benefit Stating side effects that are not risks to the patient, eg nystagmus Nonspecific, poor phrasing
2. SAQ 27 (C) Her father consents to ketamine to facilitate nasal foreign body removal. Despite the earlier midazolam, she remains anxious and is moving too much for safe insertion of a peripheral intravenous catheter. How would you prescribe (route and dose in mg) the ketamine for procedural sedation in this situation? (1 mark) Ketamine IM 80 mg (accepted range 3-5mg/kg)
2. SAQ 27 (C) Her father consents to ketamine to facilitate nasal foreign body removal. Despite the earlier midazolam, she remains anxious and is moving too much for safe insertion of a peripheral intravenous catheter. How would you prescribe (route and dose in mg) the ketamine for procedural sedation in this situation? (1 mark) Common mistake Not stating dose in mg Requirement explicitly stated in question Weight of child also listed in stem
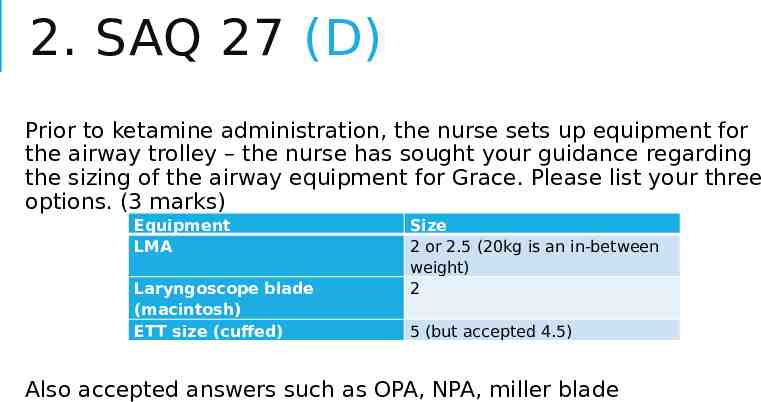
2. SAQ 27 (D) Prior to ketamine administration, the nurse sets up equipment for the airway trolley – the nurse has sought your guidance regarding the sizing of the airway equipment for Grace. Please list your three options. (3 marks) Equipment LMA Laryngoscope blade (macintosh) ETT size (cuffed) Size 2 or 2.5 (20kg is an in-between weight) 2 5 (but accepted 4.5) Also accepted answers such as OPA, NPA, miller blade
2. SAQ 27 (D) Prior to ketamine administration, the nurse sets up equipment for the airway trolley – the nurse has sought your guidance regarding the sizing of the airway equipment for Grace. Please list your three options. (3 marks) Common mistakes Putting 2 types of supraglottic devices Forgetting laryngoscope Not including sizing zero marks Incorrect sizing Using adult sizes Re: OPAs and NPAs -- if unsure of colour-coding or numeric code, safer to describe how to measure for correct size
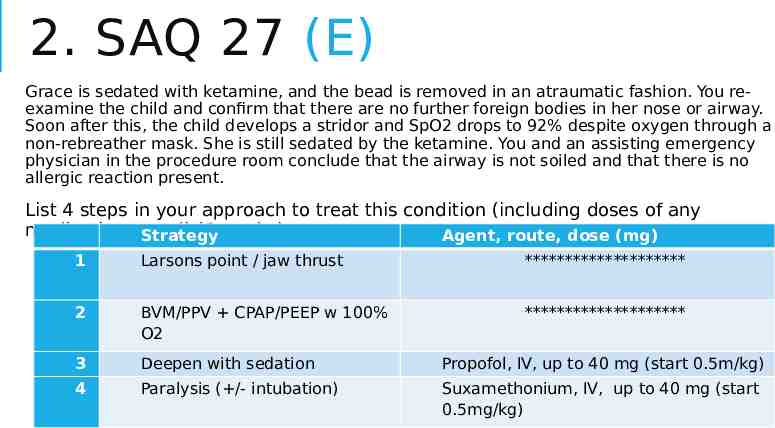
2. SAQ 27 (E) Grace is sedated with ketamine, and the bead is removed in an atraumatic fashion. You reexamine the child and confirm that there are no further foreign bodies in her nose or airway. Soon after this, the child develops a stridor and SpO2 drops to 92% despite oxygen through a non-rebreather mask. She is still sedated by the ketamine. You and an assisting emergency physician in the procedure room conclude that the airway is not soiled and that there is no allergic reaction present. List 4 steps in your approach to treat this condition (including doses of any medications Strategy used) (6 marks) Agent, route, dose (mg) 1 Larsons point / jaw thrust ******************** 2 BVM/PPV CPAP/PEEP w 100% O2 ******************** 3 Deepen with sedation Propofol, IV, up to 40 mg (start 0.5m/kg) 4 Paralysis ( /- intubation) Suxamethonium, IV, up to 40 mg (start 0.5mg/kg)
2. SAQ 27 (E) Grace is sedated with ketamine, and the bead is removed in an atraumatic fashion. You re-examine the child and confirm that there are no further foreign bodies in her nose or airway. Soon after this, the child develops a stridor and SpO2 drops to 92% despite oxygen through a nonrebreather mask. She is still sedated by the ketamine. You and an assisting emergency physician in the procedure room conclude that the airway is not soiled and that there is no allergic reaction present. List 4 steps in your approach to treat this condition (including doses of any medications used) (6 marks) Common mistakes Steps being too similar to each other, eg two steps both on positioning / airway maneouvres Treating things already excluded in stem / repeating already given treatment Not putting route of administration for medications, when multiple methods possible, eg suxamethonium ?Use of ketamine to deepen sedation Clarified with FANZCA May not work, as airway reflexes maintained Ketamine suspected to have caused the laryngospasm /- hypersalivation may be contributing
3. COHORT ANALYSIS SAQ 27 – 18 marks Pass mark 11/18 Highest mark 13.5/18 Lowest mark 0 Pass rate 27.5% Pass 11/40 Borderline 8/40 (ie within 1 mark) Fail 21/40
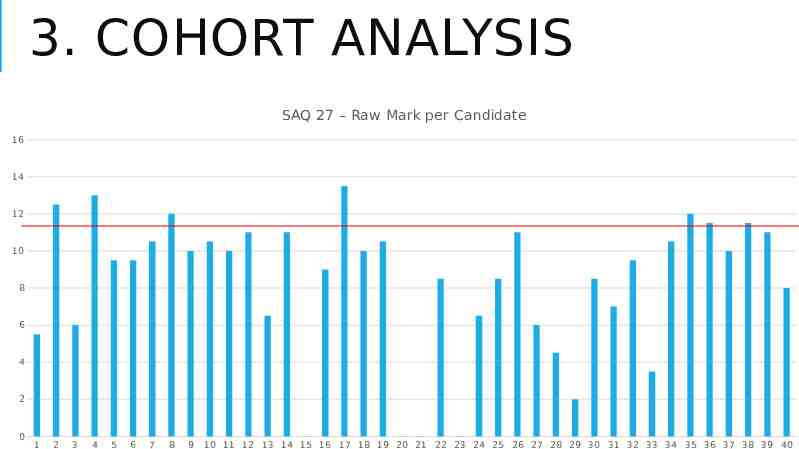
3. COHORT ANALYSIS SAQ 27 – Raw Mark per Candidate 16 14 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
4. RE-CAP / GENERAL FEEDBACK This is a game Exam performance performance as doctor Learn and play by the rules of the game, or you will not win, eg Be specific enough but not overwriting, having breadth in answer Give irrefutable answers Train hard Performance drops on exam day, multifactorial Make it harder for yourself with trial questions and exams Sleep deprived At the end of the day Quality quantity Cramming makes you feel better, but not effective Focus and fix (common) mistakes THEN move onto the next thing Personal exp: going through (review, dissect, work on gaps/weaknesses) trial questions/exams took 3x as long as actually doing the trial exam itself
5. QUESTIONS / COMMENTS? All the very best! Embrace the journey Contact Ben via benjamin.cheung@monashheal th.org Ask Ananth or Pourya