MINISTRY OF LABOUR & SOCIAL SECURITY DIRECTORATE GENERAL OF OHS Dr.
29 Slides823.50 KB
MINISTRY OF LABOUR & SOCIAL SECURITY DIRECTORATE GENERAL OF OHS Dr. Buhara Önal OHS INSTITUTE (ISGUM) May 2010 Ankara - TURKEY
CONTENT Definition of occupational health ILO/WHO Joint Committee Definition of Occupational Disases List of Occupational Diseases OH situation in Turkey
DEFINITION OF OCCUPATIONAL HEALTH JOINT ILO/WHO COMMITTEE,1950 the promotion and maintenance of the highest degree of physical, mental and social wellbeing of workers in all occupations; the prevention amongst workers of departures from health caused by their working conditions; the protection of workers in their employment from risks resulting from factors adverse to health; the placing and maintenance of the worker in an occupational environment adapted to his physiological and psychological capabilities, and to summarize: the adaptation of work to man and of each man to his job.
OCCUPATIONAL HEALTH OBJECTIVES JOINT ILO/WHO COMITTEE, 1995 the maintenance and promotion of workers’ health and working capacity; the improvement of the working environment and work to become conducive to safety and health; development of work organization and working culture in a direction which supports health and safety at work and in doing so also promotes a positive social climate and smooth operation which may enhance productivity of an undertaking.
THE EUROPEAN COMMISSION STRATEGY FOR SAFETY AND HEALTH It adopts a global approach of well-being at work taking into account the changes in the world of work and the emergence of new risks, especially of psycho-social nature. This strategy aims at promoting “well-being at work” – physical, moral and social well-being, and not just something which can be measured by absence of accidents and occupational illness. This strategy clearly suggests that health at work should not be measured only based on the number of rate of occupational diseases and accidents.
EUROPEAN AGENCY FOR SAFETY AND HEALTH AT WORK (OSHA) OHS concept includes any measures aimed at adapting work to the individual worker in order to: reduce the harmful effect of work on the individual’s health; ensure that people that have health problems are not unnecessarily excluded from the workplace or labour market as a result of work requirements and work capacities; and promote working conditions and work organization in a way that improves general health.
OCCUPATIONAL DISEASES
OHS DATA IN THE WORLD AND EU ILO Total Workforce Work related deaths Occupational accidents Occupational diseases Total Cost OSHA Work related deaths Lost working day Total ost 2.8 billion 2.2 million 270 million 160 million 30 000 billion 5.500 149 million 20 billion
DEFINITION OF OCCUPATIONAL DISEASE The term “occupational disease” covers any disease contracted as a result of an exposure to risk factors arising from work activity (the Protocol of 2002 to the OSH Convention, 1981). The ILO Employment Injury Benefits Recommendation, defines occupational diseases as following terms: “Each Member should, under prescribed conditions, regard diseases known to arise out of the exposure to substances and dangerous conditions in processes, trades or occupations as occupational diseases.”
DEFINITION OF OCCUPATIONAL DİSEASE Two main elements are present in the definition of an occupational disease: - the causal relationship between exposure in a specific working environment or work activity and a specific disease; and - the fact that the disease occurs among a group of exposed persons with a frequency above the average morbidity of the rest of the population.
GENERAL CRITERIA FOR IDENTIFICATION AND RECOGNITION OF OD The causal relationship is established on the basis of clinical and pathological data, occupational background and job analysis, identification and evaluation of occupational risk factors and of the role of other risk factors. Epidemiological and toxicological data are useful for determining the causal relationship between a specific occupational disease and its corresponding exposure in a specific working environment or work activity. As a general rule, the symptoms are not sufficiently characteristic to enable an occupational disease to be diagnosed as such without the knowledge of the pathological changes engendered by the physical, chemical, biological or other factors encountered in the exercise of an occupation.
GENERAL CRITERIA FOR IDENTIFICATION AND RECOGNITION OF OD It is therefore normal that, as a result of improvements in knowledge regarding the mechanisms of action of the factors in question, the steady increase in the number of substances employed, and the quality and variety of suspected agents, it becomes more and more feasible to make an accurate diagnosis, while the range of diseases recognized as occupational in origin is broadening.
GENERAL CRITERIA FOR IDENTIFICATION AND RECOGNITION OF OD - Strength of association. The greater the impact of an exposure on the occurrence or development of a disease, the stronger the likelihood of a causal relationship. - Consistency. Different research reports have generally similar conclusions. - Specificity. Exposure to a specific risk factor results in a clearly defined pattern of disease or diseases. - Temporality or time sequence. The exposure of interest preceded the disease by a period of time consistent with any proposed biological mechanism. - Biological gradient. The greater the level and duration of exposure, the greater the severity of diseases or their incidence. - Biological plausibility. From what is known of toxicology, chemistry, physical properties or other attributes of the studied risk or hazard, it makes biological sense to suggest that exposure leads to the disease. - Coherence. A general synthesis of all the evidence leads to the conclusion that there is a cause–effect relationship in a broad sense and in terms of general common sense. - Interventional studies. Sometimes, a primary preventative trial may verify whether removing a specific hazard or reducing a specific risk from the working environment or work activity eliminates the development of a specific disease or reduces its incidence.
CRITERIA FOR IDENTIFICATION AND RECOGNITION OF AN INDIVIDUAL DISEASE Important elements for the determination of a causal relationship: - the exposure–effect relationship (relation between exposure and the severity of the impairment in the subject) - the exposure–response relationship (connection between exposure and the relative number of subjects affected) Research and epidemiological studies have greatly contributed in this respect. Better knowledge of the causal relationship has allowed us to achieve a better medical definition of occupational diseases. As a consequence, the legal definition of occupational diseases, which was rather a complex problem, is becoming more and more linked to the medical definition and criteria.
CRITERIA FOR IDENTIFICATION AND RECOGNITION OF AN INDIVIDUAL DISEASE Legal provisions on compensation for victims vary from country to country. The Employment Injury Benefits Convention which indicates the various possibilities regarding the form of the identification and recognition of OD entitling workers to compensation benefits, states that: Each Member shall: (a) prescribe a list of diseases, comprising at least the diseases enumerated in the Convention, which shall be regarded as OD under prescribed conditions; or (b) include in its legislation a general definition of OD broad enough to cover at least the diseases enumerated in the Convention; or (c) prescribe a list of diseases in conformity with clause (a), complemented by a general definition of OD or by other provisions for establishing the occupational origin of diseases not so listed or manifesting themselves under conditions different from those prescribed.
CRITERIA FOR IDENTIFICATION AND RECOGNITION OF AN INDIVIDUAL DISEASE The “list system” covers only a certain number of occupational diseases, and has the advantage of listing diseases for which there is a presumption that they are of occupational origin. This simplifies the matter for all parties since it is frequently very difficult, if not impossible, to prove or disprove that a disease is directly attributable to the victim's occupation. It also has the important advantage of indicating clearly where prevention should focus. The “general definition system” theoretically covers all occupational diseases; it affords the widest and most flexible protection, but leaves it to the victim to prove the occupational origin of the disease. In practice, it also often implies that arbitration on individual cases is necessary. Furthermore, no emphasis is placed on specific prevention. The “mixed system” has been favoured by many ILO member States, because it combines the advantages of the other two without their disadvantages.
CRITERIA FOR INCORPORATING A DISEASE INTO THE ILO LIST OF OCCUPATIONAL DISEASES The List of Occupational Diseases Recommendation, 2002 (No. 194) was adopted at the 90th Session of the International Labour Conference, 2002. The Committee on Occupational Accidents and Diseases established in 2002 to work on the List of Occupational Diseases Recommendation requested the Governing Body of the International Labour Office to convene the first of the tripartite meetings of experts referred to the Recommendation as a matter of priority. The Committee expected that, in addition to examining the Annex to the Recommendation, the existing national and other lists of occupational diseases, and the comments received from member States, the Meeting should consider all the amendments submitted on the Annex to the Conference Committee.
UPDATING THE LIST OF OD Decisions to incorporate specific diseases in the updated List of OD need to take into account the following general criteria: - there is a causal relationship with a specific agent, exposure or work process; - they occur in connection with the work environment and/or in specific occupations; - they occur among the groups of persons concerned with a frequency which exceeds the average incidence within the rest of the population; and - there is scientific evidence of a clearly defined pattern of disease following exposure and plausibility of cause.
LIST OF OCCUPATIONAL DISEASES (ILO) 1. Diseases caused by agents 1.1. Diseases caused by chemical agents 1.2. Diseases caused by physical agents 1.3. Diseases caused by biological agents 2. Diseases by target organ systems 2.1. Occupational respiratory diseases 2.2. Occupational skin diseases 2.3. Occupational musculo-skeletal disorders 3. Occupational cancer 3.1. Cancer caused by the following agents 4. Other diseases 4.1. Miners' nystagmus
OCCUPATIONAL HEALTH IN TURKEY A COUNTRY PROFILE
DEMOGRAPHIC CHARACTERISTICS, TURKEY 780 000 sq. km. population 71 million, 65% live in urban area Age: 15 %20; ---- 65 %5.7 M % *** -------- F % *** Total workforce 26 million
SGK STATISTICS (2008) 1.170.248 workplaces 8.802.989 compulsory insured person 72.963 539 866 occupational accidents occupational diseases deaths due to occupational accidents and occupational diseases
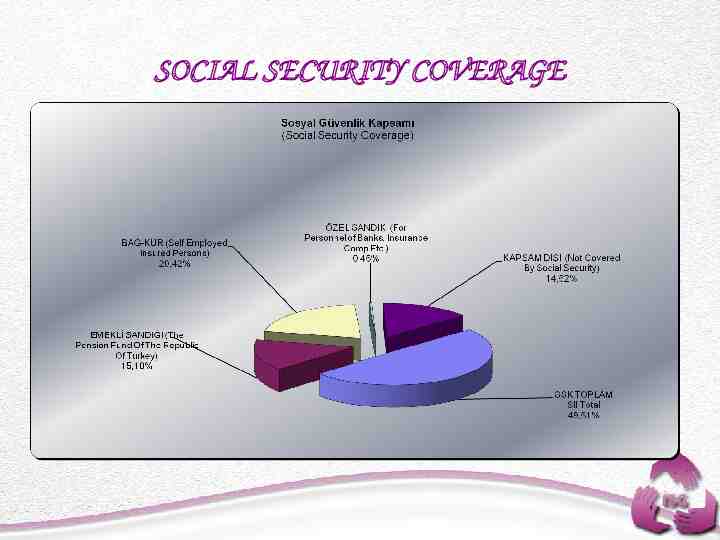
SOCIAL SECURITY COVERAGE
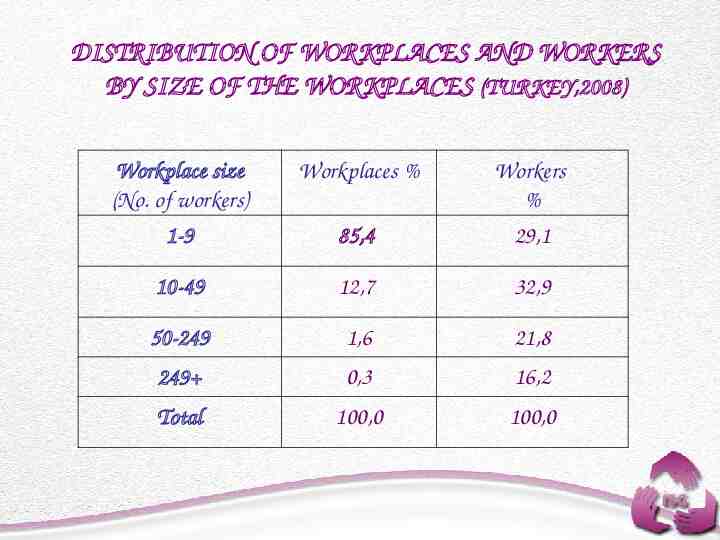
DISTRIBUTION OF WORKPLACES AND WORKERS BY SIZE OF THE WORKPLACES (TURKEY,2008) Workplace size (No. of workers) Workplaces % Workers % 1-9 85,4 29,1 10-49 12,7 32,9 50-249 1,6 21,8 249 0,3 16,2 Total 100,0 100,0
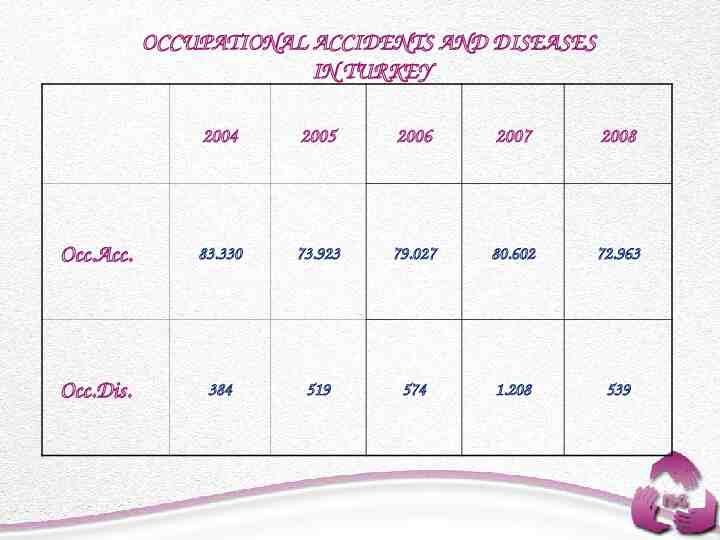
OCCUPATIONAL ACCIDENTS AND DISEASES IN TURKEY 2004 2005 2006 2007 2008 Occ.Acc. 83.330 73.923 79.027 80.602 72.963 Occ.Dis. 384 519 574 1.208 539
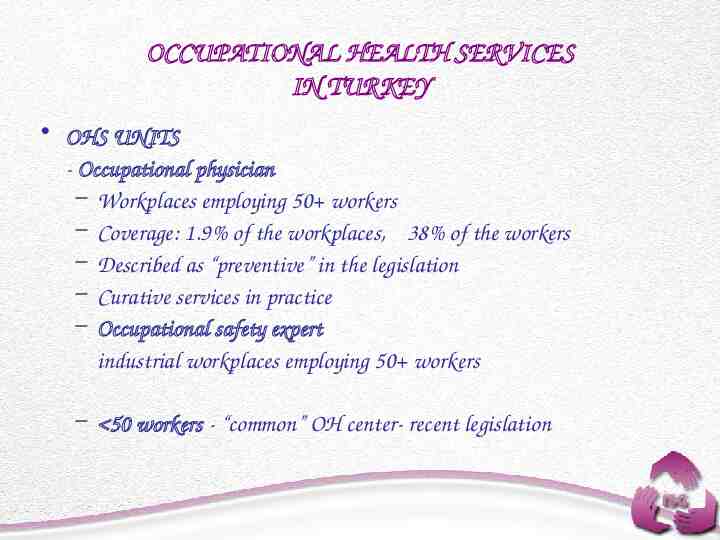
OCCUPATIONAL HEALTH SERVICES IN TURKEY OHS UNITS - Occupational physician – Workplaces employing 50 workers – Coverage: 1.9% of the workplaces, 38% of the workers – Described as “preventive” in the legislation – Curative services in practice – Occupational safety expert industrial workplaces employing 50 workers – 50 workers - “common” OH center- recent legislation
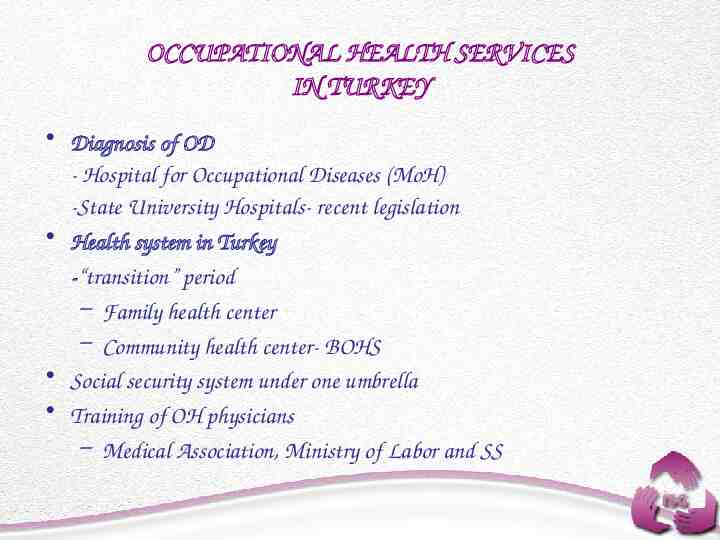
OCCUPATIONAL HEALTH SERVICES IN TURKEY Diagnosis of OD - Hospital for Occupational Diseases (MoH) -State University Hospitals- recent legislation Health system in Turkey -“transition” period – Family health center – Community health center- BOHS Social security system under one umbrella Training of OH physicians – Medical Association, Ministry of Labor and SS
THANK YOU Dr. Buhara ÖNAL [email protected] 00 90 312 2571690/200